Orthopedic Devices
|
Conservative Fracture Treatment |
|
|
|
|
|
|
|
|
|

|
Fracture Fixation
by Tim B Hunter, MD, MSc
Conservative Fracture Treatment
Conservative fracture treatment consists of
closed reduction to restore bone alignment and produce bone and soft tissue stabilization. It is achieved either by external splinting (splints and casts) or by external or internal traction (Ruedi, 2007; Benjamin, 1994; Wiss, 2013; Berquist, 1995; Freiberg, 2001; Hunter, 2001).
Casts and splints
External fracture immobilization by casts and splints is an everyday occurrence. Large splints composed of metal, airbags, or plastic have been developed to immobilize fractures in the femur and other large bones (figure: femur fracture splinting and traction) (figure: hinged knee brace). Somewhat smaller plaster and metallic splints stabilize fractures in the arm, forearm, hand and wrist, tibia and fibula, and ankle and foot (figure: wrist splint). There are small metallic splints for finger and toe fractures. Specialized splints have even been developed for particular finger and toe injuries (figure: dorsal blocking splint).
Casts and splints are composed of many materials, including plaster of Paris, synthetic casting material, and metal. Plaster of Paris is most frequently used to make splints and casts, because it is inexpensive, easy to mold, "breathable," and absorbent (figure: plaster cast). Synthetic casting materials are lighter and stronger, but they are more expensive and non-absorbent (figure: fiberglass cast).
Casts and splints can be used either for temporary immobilization of an extremity, or they can be used for definitive treatment of an extremity fracture. They are often combined with internal fixation to provide additional support and protection of the extremity. Braces are also used to limit the range of motion of a joint after surgery or after trauma. In many cases, percutaneous pins ("Kirschner or K-wires") (figure: K-wires) are used in combination with a plaster cast to achieve treatment similar to an external fixator, so-called "pins in plaster" (figure: pins in plaster).
External and internal traction devices
Skeletal traction is the pulling on a bone through a pin or wire inserted into the bone. The pulling is used to reduce and stabilize a fracture. It is most commonly used in the lower extremity. Traction devices are applied along
the long axis of the bone. They align the bone
fragments and provide a degree of stability (figure: traction pin) (figure: femur fracture splinting and traction).
Traction devices work only when the bone fragments are still connected to soft tissues. Skeletal
traction entails the insertion of either a Kirschner (K)-wire or Steinman pin through the bone. The Kirschner wire has a smaller diameter and produces less injury to the soft tissues than does the Steinman pin, but it requires the use of a tensioned traction bow. Steinman pins come in a variety of sizes. Both Kirschner wires and Steinman pins can be smooth, partially threaded, or fully threaded. The threaded pins are associated with a more traumatic insertion than smooth pins, but they are less likely to loosen over time.
The most common indication for skeletal traction is a femoral fracture (figure: femur fracture traction). Less commonly, skeletal traction is used for humeral fractures as well as some other lower extremity fractures and dislocations. Sometimes, intraoperative skeletal traction is used for the reduction of a distal radius fracture (Ruedi, 2007; Wiss, 2013).
Traction pins for the lower extremity are placed in one of three sites: supracondylar femur, proximal tibia, or in the calcaneus. Possible complications
with supracondylar traction are quadriceps injury, neurovascular injury, and infection. Calcaneal traction, while not uncommon, should ideally be avoided, because it has a high infection rate (figure: calcaneal traction). When a traction pin, fixation pin, or fixator pin has been removed from the bone, a lucent, hollow cylindrical track is left in the bone, a so-called ghost tract (figure: calcaneal ghost tract). The indications, technique, and complications with lower extremity traction pins are nicely summarized by Althausen and Hak (Althausen, 2002).
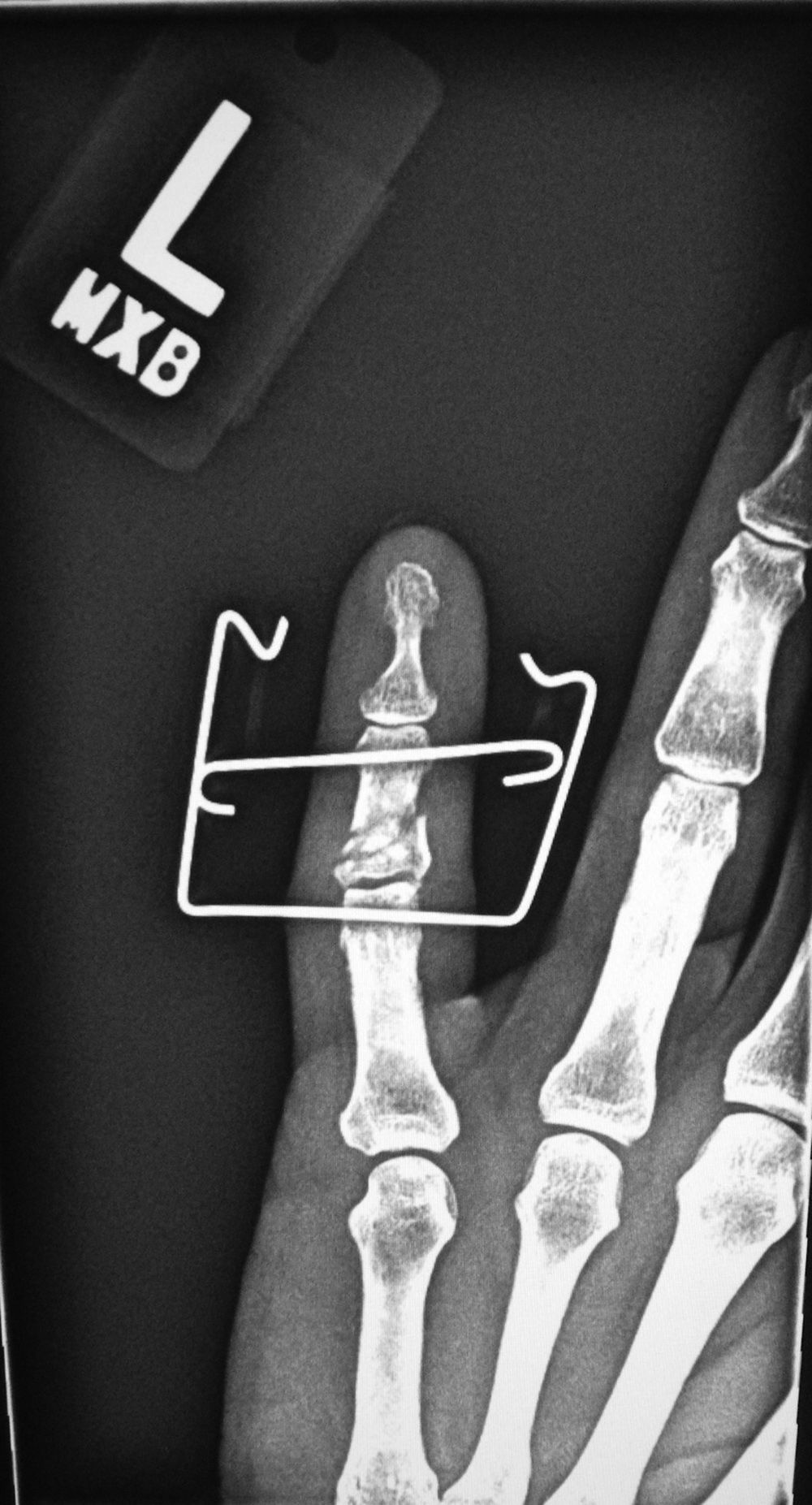
The Suzuki frame and Suzuki fixator are specialized devices for reducing and stabilizing complex intra-articular finger fractures. Rubber bands generate traction between two K-wires placed into the bone on either side of the fracture (figure: Suzuki frame; figure: Suzuki fixator). Other specialized traction devices are also used for finger and wrist traction (figure: finger traction).
Back to Top
External Fixation
An external fixator is an externally applied device with bone screws or pins designed for the stabilization and immobilization of open long bone fractures. It provides fracture fixation based on the principle of splinting. External fixators are the only system that allows the surgeon to control the flexibility of the fixation. External fixators are the standard in treating open fractures with substantial soft-tissue injuries that require vascular procedures, fasciotomy, soft-tissue flaps, or multiple debridements to avoid additional damage to an already compromised limb.
The other indications for the application of an external fixator are polytrauma; fractures in children to avoid pin fixation through the growth plate; temporary joint bridging before later open reduction and internal fixation (ORIF); and arthrodesis of the ankle, elbow, or knee. In these latter cases, external fixators are especially indicated in acute or chronic infections, in limb-lengthening procedures, and occasionally after corrective osteotomies (Ruedi, 2007; Benjamin, 1994; Wiss, 2013; Berquist, 1995; Freiberg, 2001; Hunter, 2001).
External fixators are made of connecting rods with pins, screws, or wires (Schanz screws, Steinman pins, Kirschner wires) that are placed percutaneously into the bone above and below the fracture site. These pins, screws, or wires are connected by various clamps to the external fixation rods which are composed of stainless steel or carbon fiber.
There are three basic types of external fixators: a) standard pin (or uniplanar) fixator (figure: external fixator radius; figure: Stableloc external fixator), b) ring fixator (figure: ring fixator), and c) hybrid fixator (figure: hybrid fixator). Standard uniplanar external fixators consist of percutaneously placed pins that are connected to an external
rod. Proper pin or screw placement is very important. These pins or screws should penetrate the near cortex and medullary canal and engage the far cortex without penetrating the muscle compartment. Joint penetration by any of these pins must be avoided. Standard uniplanar fixators can be used for almost every long bone fracture except those involving the proximal femur or humerus. They are commonly used for the stabilization of complex distal radius fractures. The pins are placed in the distal radius and second metacarpal shaft. This technique uses the surrounding soft tissues or ligaments to provide indirect
stabilization of the fracture. Uniplanar external fixators have a limited use in temporary stabilization of pelvic fractures (figure: uniplanar pelvis external fixator).
Ring fixators are made of thin wires under tension that are attached to circular or semicircular rings or frames. This technique was introduced by the Russian surgeon Ilizarov for limb-lengthening procedures. Currently, it has broader applications. The term Ilizarov fixator is frequently
used for any type of ring fixator (figure: ring fixator) (Ruedi, 2007; Benjamin, 1994; Berquist, 1995; Freiberg, 2001; Hunter, 2001).
The third type of external fixator is called a hybrid fixator (figure: hybrid external fixator). It represents the combination of ring and standard uniplanar fixators. It is commonly used for treatment of the proximal and distal tibial fractures that are close to the joint.
This fixator is made of a 3/4 ring proximally, which is attached to the bone by Kirschner wires. The ring is connected to a unilateral external rod, which is attached to the distal bone shaft by Schanz screws.
The adequate care of pin-track sites is important and starts at the day of placement. Daily cleansing and disinfection is necessary to minimize pin-track infection. Radiography is used to evaluate for pin loosening, breakage, and infection. Visualization of the entire device is frequently limited because of the overlapping frame, and additional views and even fluoroscopic evaluation may be needed for adequate assessment of possible complications (Ruedi, 2007; Benjamin, 1994; Wiss, 2013; Berquist, 1995; Freiberg, 2001; Hunter, 2001).
Pinless fixators are sometimes used for tibial fractures but they are less stable. With these fixators, the medullary canal is not penetrated because
the clamps (forceps) are anchored into the cortex only. This type of fixation allows later safe intramedullary nailing (Ruedi, 2007).
Back to Top
Back to Top
|