Complications
|
|
Joint Arthroplasty Complications |
|
|
|

|
Complications of Joint Arthroplasty
by Jason R Wild, MD
Complications of Joint Arthroplasty
Introduction
In contrast to fracture fixation devices, arthroplasty implants are designed to bear load indefinitely while allowing for motion of the joint. They are therefore not only susceptible to failure, such as breaking or loosening, but because of the joint articulation, are also susceptible to dislocation and wear of the joint bearing surfaces. Arthroplasty implants achieve bone fixation by a) friction fit, where they are pressed into the bone; b) by in-growth where the bone grows into their surfaces; c) by cement fixation; d) by fixation with screws; or e) by a combination thereof (Gelman, 1984; Benjamin, 1994; Berquist, 1995; Freiberg, 2001).
Close inspection of the implant/bone interface can reveal loosening. It may appear as a halo surrounding the implant where motion is occurring or where fluid is present (figure: failure of radial head prosthesis; figures: implant loosening with osteolysis). A unique type of failure seen in arthroplasty occurs when wear of the bearing surface releases small polyethylene particles. These particles, by nature of their size and shape can induce an inflammatory response. As phagocytes attempt to digest these particles, they release lytic enzymes which lead to osteolysis. This is sometimes termed “particle disease,” and is characterized by significant lytic lesions surrounding the implant (figure: particle disease in right hip; figure: particle disease in left hip) (Galante, 1998; Awan, 2013; Mulcahy, 2012; Mulcahy, 2014).
Natural wear of the bearing surface does not always cause loosening or failure of the implant but may be a source of concern. As the bearing surface wears out, it becomes thinner and can eventually crack or wear through. Once the bearing surface has worn through, it can cause wear of the underlying metal components which may necessitate total component revision or it may induce particle disease. If the wear is identified in a timely manner, the condition may be treatable by simply exchanging the bearing surface, rather than a complete revision. Wear is detected best on weight bearing radiographs which may show a change in the expected joint space or an asymmetrical joint space on plain radiographs (figure: polyethylene liner wearing; figure: polyethylene liner displacement). Comparison with previous radiographs is essential. It may be difficult to distinguish between polyethylene linear wearing and liner displacement. The distinction is somewhat moot as in either case the liner has to be replaced and possibly the entire arthroplasty revised.
Wear of polyethylene has seen some interesting changes in orthopedic history. After attempting gamma-irradiation in air as a means for sterilization of the polyethylene, accelerated wear was observed. This method of sterilization leads to oxidation of the polyethylene, weakening the connection between molecules. This leads to rapid delamination failure of the polyethylene. Newer manufacturing and sterilization methods to reduce oxidation, and to increase molecular cross-linking have dramatically improved polyethylene wear.
Metal-on-metal implants have gained a lot of publicity secondary to a statistically rare complication termed metal-on-metal disease (Bestic, 2013; Ardaugh, 2013). Small particles of metal are released with wear and these can induce local and systemic reactions. Metal ion levels (cobalt or chromium) in the blood may reach very high concentrations during this disease and are used for diagnosis. Similar to normal polyethylene wear, the metal particles can cause implant loosening through release of lytic enzymes by macrophages (Bradberry, 2014; Reito, 2014; Visuri, 2010).
Back to Top
Arthroplasty Dislocation
Dislocation of prosthetic joints is particularly troublesome for the patient and the treating surgeon (figure: right total shoulder arthroplasty anterior dislocation; figure: posterior reverse total shoulder arthroplasty dislocation; figures: hip arthroplasty dislocations). The placement of arthroplasty components, by definition, requires dislocation of the native joint. In doing so, soft tissue releases are often required. The lack of native stability by the soft tissue or bony articulation may lead to dislocation.
Dislocation risk can be altered by several patient and surgeon related factors. Component position is often the most important variable for arthroplasty stability. It can be evaluated radiographically and should be carefully studied (Manaster, 1996; Mucahly, 2012). Other factors, such as patient compliance and co-morbidities, require a careful chart review and direct patient examination to establish the underlying risk for possible arthroplasty dislocation.
Detection of an arthroplasty dislocation is most easily performed by comparison of the arthroplasty's radiographic appearance with immediate postoperative radiographs which usually have a reduced joint. AP radiographs may demonstrate subtle changes for a dislocated joint. If the prosthetic joint is dislocated anteriorly further from the radiographic cassette, the implant will appear larger than usual. Vice versa, if the prosthetic joint is dislocated posteriorly closer to the radiographic cassette, it will appear smaller than usual.
The load bearing surface of an arthroplasty may dislocate from the prosthesis (figure: polyethylene liner displacement). Most bearing surfaces are polyethylene and are radiolucent. Many manufacturers place a metal tag within the polyethylene components to help identify their position radiographically (figure: knee arthroplasty with metallic polyethylene locking clip). However, dissociation of the polyethylene can be extremely difficult to detect. In cases of liner dissociation the joint often does not appear concentrically reduced, and the periarticular soft tissues appear irregular. Soft tissue shadows may reveal the displaced radiolucent polyethylene (figure: right hip dislocation with polyethylene liner displacement).
Back to Top
| Right shoulder hemiarthroplasty failure with loosening and osteolysis |
|
 |
 |
 |
|
| 53 year-old man in motorcycle accident. Initial radiograph shows a comminuted fracture of the proximal right humerus with dislocation of the humeral head (left image). The fracture was treated with a right shoulder hemiarthroplasty (center image). At follow-up 6 months later there was failure of fracture healing with associated hardware loosening and osteolysis (arows on right image). Images courtesy Laura H Lee, MD. |
|
 |
| Right bipolar radial head prosthesis with eventual prosthesis loosening |
 |
 |
 |
 |
| 57 year-old woman with radial head prosthesis and capitellar suture anchor. In 2011 she had a right elbow dislocation with a comminuted radial head fracture. A bipolar radial head prosthesis was placed to treat post-traumatic arthritis. Initial radiographs obtained in 2014 (left two images) showed the prosthesis to be well seated. Later radiographs in 2015 show prominent periprosthetic lucency around the prosthetic stem indicating non-infectious aspetic loosening. There are also chronic fractures of the proximal portions of the right radius and ulna. |
|
| Infected total elbow arthroplasty with eventual placement of a revision total elbow arthroplasty |
 |
 |
 |
 |
| 66 year old man with infected left elbow arthroplasty. The arrows point to areas of periprosthetic lucency suggesting loosening which was found to result from an infected prosthesis. The patient had the prosthesis removed and underwent multiple subsequent surgeries with placement of a revision elbow arthroplasty. |
|
| Focal osteolysis about femoral stem of total hip arthroplasty |
Femoral osteolysis and loosening of noncemented total hip arthroplasty |
Right ankle prosthesis failure with loosening of components and polyethylene wear medially |
Right hip arthroplasty polyethylene wear |
 |
 |
 |
 |
| Cemented total hip arthroplasty with focal osteolysis about the stem in zones, 2, 5, and 7. From Benjamin, 1994 |
There is radiolucency (arrow) around the entire femoral stem with a sclerotic margin. There is also thinning of the lateral femoral cortex. From Benjamin, 1994 |
68 year-old woman with total ankle prosthesis failure with loosening of tibial and talar component shown by bony lucency about the components and medial polyethylene liner wearing. |
|
|
| Displaced polyethylene liner in right hip arthroplasty |
Right hip dislocation with displaced polyethylene liner |
 |
 |
 |
 |
| Image courtesy Lana Hirai Gimber, MD |
Initial AP radiograph (left) shows a right hip dislocation. Note the polyethylene liner (arrow) is still associated with dislocated femoral head. The hip was subsequently relocated. The AP radiograph (middle) show subtle eccentric positioning of the reduced femoral head within the acetabular cup. A subtle density (arrows) represents the liner which is now disassociated from the femoral head. This is somewhat more clearly shown (arrow) on the frog leg lateral view (right). |
|
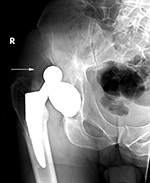
| Osteolysis and particle disease in right hip replacement |
Particle disease (arrows) left hip coronal CT image |
|
 |
 |
 |
|
|
|
68 year-old man with particle disease from a worn out left hip prosthesis. Bony destruction (arrows) is in the left supra-acetabular region and in the left greater trochanter with a pathologic fracture. |
|
|
| Right shoulder hemiarthroplasty anterior dislocation |
Posterior dislocation of a reverse total shoulder arthroplasty |
 |
 |
 |
 |
| |
|
|
|
|
| Semiconstrained left elbow arthroplasty with heterotopic bone formation |
Left elbow semiconstrained prosthesis with olecranon periprosthetic fracture |
|
 |
 |
 |
|
| 35 year-old woman with prior gunshot injury to left upper extremity. Multiple surgeries were performed to remove wooden fragments and shrapnel. Extensive heterotopic bone has developed about the left humerus and left elbow arthroplasty. Portions of previous fixation screws and plates are evident. |
|
|
|
| Disrupted wrist prosthesis |
Second generation total wrist arthroplasty and Silastic metacarpophalangeal (MCP) implants. |
Third generation "biaxial" total wrist prosthesis |
 |
 |
 |
 |
| Elderly woman with advanced rheumatoid arthritis. Swanson silicone joint prostheses are present at the right 1st, 2nd, and 3rd metacarpophalangeal joints, and Herbert-like screws are at the proximal interphalangeal joints of the right 2nd, 3rd, and 4th fingers. The Swanson silicone prosthesis at the wrist radiocarpal joint has become completely disrupted with displacement of the radial component. |
The wrist is malaligned in ulnar deviation. There is extensive remodeling in the long (3rd) finger metacarpal. Metal grommets with Silastic implants are at the thumb and long finger MCP joints. From Hunter, 1994. |
52 year-old woman with rheumatoid arthritis and left total wrist prosthesis which failed three years later and was replaced by a wrist arthrodesis. The distal stem of the prosthesis protruded out of the left 3rd metacarpal. The radiograph of the left wrist arthrodesis shows 2nd-5th MCP Swanson silicone arthroplasties, most of which are at least partially displaced. On the patient's right side there are also extensive changes of rheumatoid arthritis with multiple failed Swanson silicone MCP prostheses (see the two images to the right). |
|
| Multiple failed metacarpophalangeal Swanson silicone arthroplasties |
Subtle failure of total knee arthroplasty (TKA) |
|
 |
 |
 |
|
| 52 year-old woman with severe rheumatoid arthritis in the right hand and wrist. There are multiple failed MCP Swanson silicone prostheses with partial displacement and bone fracturing. There is surgical arthrodesis at the right index finger MCP joint and bony fusion from long standing arthritis in the wrist and thumb MCP joint. In her left hand and wrist there was failure of a wrist prosthesis and failure of MCP joint arthroplasties (see the two images to the left). |
A noncemented total knee arthroplasty is present with a metal backed patellar component. There is also a polyethylene locking clip which locks the tibial polyethylene into the tibial base plate. The anterior cortex of the femur is notched and eroded (top arrow). There is also subtle subsidence of the tibial component (bottom arrow). From Benjamin, 1994 |
|
|
| Disrupted left total knee prosthesis |
Failed constrained total knee arthroplasty from destructive particle disease |
 |
 |
 |
 |
| |
|
96 year-old woman with destructive particle disease causing large areas of bone destruction (arrows). |
Back to Top
Shoulder prostheses come in a variety of flavors: hemiarthroplasty, total shoulder arthroplasty (TSA), and reverse total shoulder arthroplasty (RTSA). In hemiarthroplasty the humeral component articulates with the patient’s native glenoid. In total arthroplasties, both sides of the joint are replaced. The standard total shoulder prosthesis maintains an anatomic appearance, whereas the reverse total shoulder prosthesis places a sphere on the glenoid and a concave bearing surface on the humeral side (Roberts, 2007; Petscavage, 2012; Ha, 2012).
RTSA has a unique mode of loosening termed scapular notching. This is present at the inferior aspect of the glenoid near the implant/bone interface. It is thought to be caused by mechanical wear as the humeral component contacts the inferior glenoid. Newer component design and better placement recommendations have decreased the incidence of scapular notching (figure: left reverse total shoulder arthroplasty with scapular notching).
The initial postoperative radiographs frequently show thin radiolucent areas about the prosthesis, particularly
about the cemented glenoid component. In most cases they are likely related to difficulty in achieving good
cement penetration into the bone and are of no consequence. However, on subsequent
radiographs there should be no progression of any radiolucent lines at the implant-
bone interfaces, since they may indicate loosening and/or infection (figure: right shoulder hemiarthroplasty failure).
The main complications seen with shoulder
arthroplasty are loosening and subluxation or dislocation.
Periprosthetic humeral shaft fractures
can occur intra-operatively or after surgery secondary
to trauma (Lazarus, 2002; Boileau, 2002; Boileau, 2006) (figure: right shoulder prosthesis periprosthetic fracture). Relatively speaking, shoulder arthroplasty has a higher complication rate (15%) than hip or knee arthroplasty. This is likely related to the available bone stock, and the inherent mobility of the joint with a lack of bony constraint (Bohsali, 2006).
The weak link in total shoulder arthroplasty is often the glenoid component, since the scapula has little bone stock and the native glenoid has a conical shape (Schrumpf, 2011). Loosening of the glenoid component is far more common than humeral loosening. Thirty percent of primary osteoarthritis shoulder arthroplasty revisions are due to glenoid loosening (OrthoBullet).
Rocking horse loosening or failure is a term to describe eccentric loading of the prosthetic humeral head on the glenoid component in which the head rocks back and forth in a non-concentric fashion on the glenoid component. This constant uneven loading can cause failure of the glenoid component fixation to the underlying bone glenoid bone.
Elbow arthroplasty remains challenging, as the elbow is a highly constrained joint. This constraint places a higher load on the bone implant interface than on a lesser constrained joint. The forces transmitted across the elbow are amplified by the
long lever arm of the forearm, and there is limited bone stock about the elbow. In addition, this joint is actually 3 joints (proximal radioulnar, radiocapitellar, ulnohumeral) which are all required for normal forearm function.
Elbow arthroplasty comes in two flavors, linked or unlinked. Unlinked arthroplasty has no hinge, and therefore functional ligamentous structures around the elbow are imperative for joint stability. Linked varieties contain an actual hinge and have more constraint (figures: constrained and semi-constrained elbow joint arthroplasty).
The natural constraint of the native elbow joint makes it difficult to place either type of implant correctly, and it also decreases the life expectancy of the implanted joint (Inglis, 1980; Lin, 2016). Elbow arthroplasty has a higher complication rate than most other artificial joints (figure: failure of radial head prosthesis; figure: infected elbow joint prosthesis). This results from breakdown of the arthroplasty itself or from loosening of the prosthesis and chronic fracturing of the surrounding bone.
The elbow is particularly prone to heterotopic bone formation after immobilization or surgery. This complication is not uncommon after elbow prosthesis placement. It may be relatively benign, but it can lead to significant loss of joint mobility and require surgical removal (figure: semiconstrained elbow prosthesis with heterotopic bone formation).
Joint prosthesis infection is uncommon but a dreaded complication of elbow arthroplasty (figure: infected total elbow arthroplasty). Aseptic (non-infectious) prosthetic loosening is more common than prosthesis infection, but the differentiation between prosthesis infection with loosening and aseptic loosening is difficult to determine with imaging alone and may require surgical exploration if there are clinical findings suggesting an infection. While not common, periprosthetic elbow fractures may occur and should be looked for when evaluating radiographic studies of elbow prosthesis placement (figure: olecranon periprosthetic fracture).
Total wrist arthroplasty (TWA) continues to evolve as a treatment for arthritis. It remains relatively uncommon compared to other arthroplasties, mostly due to high complication rates with instability and loosening. In addition, wrist fusion is fairly well tolerated in this patient population (figures: wrist arthroplasty failures; figure: wrist arthroplasty failure with later arthrodesis; figure: failed finger arthroplasties). However, total wrist arthroplasty may be applicable in some cases, because improvements in
biomaterial technology and surgical technique have made wrist arthroplasty a good alternative for patients who might have had an arthrodesis. Wrist arthroplasty offers increased wrist function, and the more modern prostheses and surgical techniques promise less associated complications and a longer functional lifespan for the prosthesis (Nair, 2014; van Harlingen, 2011; Bales, 2014).
What is important is to realize radiocarpal arthroplasty is used in patients with end-stage destructive arthritis, usually rheumatoid arthritis, to good initial effect, but there are long term complications with osteolysis, loosening, and disruption of the prosthesis. All elbow, wrist, and finger arthroplasties suffer from these possibilities, and imaging evaluation of them should always look for early signs of prosthesis failure.
Small joint arthroplasty for hand arthritis continues to evolve. Rheumatoid patients suffer arthritis of these joints particularly. Silastic spacer implants, which serve as an interposition arthroplasty, have been used in the past with varied results. Long term data suggests improved patient satisfaction without significant functional improvement (Waljee, 2012). However, radiographic osteolysis does not always correlate with patient symptoms or satisfaction. Anatomical designed arthroplasties are being explored, and they appear to be effective for symptom relief, but loosening rates may be no better than Silastic implants.
Back to Top
Hip arthroplasty also comes in 3 different flavors. Hemiarthroplasty replaces only the femoral side, which then articulates with the native socket. This can be done with a bipolar or a unipolar component (figure: unipolar hip prosthesis). A bipolar component has an articulation between a smaller metal head and a polyethylene component which sits inside a larger metal head that articulates with the acetabulum (figure: bipolar hip prosthesis). On quick examination, this can appear similar to a total hip arthroplasty – key identifiers are the presence of a joint space between the larger metal head and the subchondral acetabular bone, the variable position of the larger head on radiographs, and the absence of screws or bone cement affixing the acetabular component to the pelvis. Without sufficient clinical information it may be difficult to distinguish between a unipolar or bipolar hemiarthroplasty.
Total hip arthroplasty (THA) replaces both the femoral head and the acetabular socket. Fixation of the acetabular side is most commonly press-fit with screw augmentation (figure: bilateral total hip arthroplasty with right hip arthroplasty dislocation). Cemented acetabular components have shown early loosening and are now essentially reserved for revision or tumor cases. Femoral-sided fixation can be achieved with cement or with press-fit fixation. Many different bearing surfaces have been tried, but the gold standard remains a metal femoral head on a polyethylene socket bearing surface. Ceramic is also used which is more dense than polyethylene but less dense than the cobalt chrome metal component (Hannouche 2016). Ceramic is prone to a unique failure mode due to its brittle nature. The ceramic component can shatter if loaded to failure. This mode of failure is particularly troublesome for the patient and treating surgeon since the fragments are razor sharp.
Resurfacing replaces the acetabulum and the femoral head while preserving the femoral neck. This is reserved for younger individuals with better bone quality and higher physical demands. Femoral neck fracture is a unique complication after this type of arthroplasty, since the neck is preserved. As resurfacing arthroplasty attempts to retain as much bone as possible, implant design is restricted to metal-on-metal components which take up less space. For this reason, resurfacing is subject to metal-on-metal particulate/ion disease.
Non-infectious (aseptic) loosening of prosthetic components is the most common cause for hip implant failure and subsequent revision surgery. The failure can occur at the prosthesis-bone interface, prosthesis-cement interface,
or cement-bone interface. Progressive development of radiolucent areas greater than 1 mm at these interfaces is worrisome for prosthesis loosening (figure: osteolysis at tip of femoral stem).
Hip and knee arthroplasty are common surgeries, far more common than other joint arthroplasty (see Joint Arthroplasty-Introduction). While no surgical procedure is without risk, hip and knee replacement are major surgical undertakings requiring considerable patient rehabilitation and recovery. Since they generally are in older patients with frequent co-morbidities, there is not a trivial risk for major postoperative complications including, bleeding, deep venous thrombosis, and infection (Visuri, 2010; Hunt, 2014; Lindgren, 2014; McCalden, 2013; Pedersen, 2014).
The infection rate may be as high as 1-2% for primary total hip replacement and even higher for total hip revision (Mulcahy, 2012; Patel, 2023). In Sweden the cumulative incidence of primary joint infection within two years after primary total hip replacement has been reported to be 0.9% with staphylococcus aureus and coagulase-negative staphylococci as the most common bacteria isolated (Lindgren, 2014).
Back to Top
Knee arthroplasty poses a challenge for detecting loosening as the components are typically flat along the bone implant interface and applied to the external surface of the bone. It is therefore particularly difficult to get a perfectly tangential radiographic view of the bone/implant interface, which is necessary to detect subtle signs of loosening (figure: knee arthroplasty failure). In contrast, hip arthroplasty components usually have a convex surface, thus every radiographic view is tangential to the bone/implant interface. In more rare occasions, there may be a total disruption of the knee arthroplasty or marked destruction from particle disease (figure: disrupted left total knee prosthesis; figure: knee prosthesis particle disease).
Knee arthroplasty components can have a variable degree of constraint to motion. Total knee arthroplasties (TKA's) going from less to greater constraint are as follows: cruciate retaining TKA, posterior stabilized TKA, varus-valgus constrained TKA, and rotating-hinge knee implants. With increasing constraint, increasing load is placed on the implant-bone interface. Posterior stabilized and varus-valgus constrained knees have a polyethylene post in the center of the tibial polyethylene tray which interfaces with a metal box in the femoral component. It is possible for the femoral component to “jump the post,” which is essentially a posterior knee dislocation. With all of the above, the anterior cruciate ligament (ACL) is sacrificed. Bi-cruciate retaining knees are essentially medial and lateral unicondylar tibial trays with a completely replaced femoral side. This allows for preservation of the ACL insertion on the tibia (figure: Biomet Vanguard bicruciate retaining TKA).
Even patients aged 90 and over may be candidates for total knee arthroplasty. They do have a greater number of co-morbidities preoperatively with a higher rate of postoperative deep vein thrombosis, a longer hospital stay, and increased 30 day mortality (Mirac, 2014).
Hematoma or seroma formation is the most common immediate postoperative complication related to knee arthroplasty. In almost all cases of orthopedic surgery in which the bone marrow is disturbed, whether fracture fixation or placement of a joint prosthesis, there is some degree of systemic fat embolism with emboli going to the lungs. Fortunately, this rarely produces fat embolism syndrome which is uncommon but occurs most often after traumatic bone fracture (Dhar, 2012; Tsai, 2010).
Long term complications associated with knee arthroplasty are similar to those seen with hip arthroplasty. They include include non-infectious aseptic
loosening from a varying combination of polyethylene wear, small particle disease, or non-specific osteolysis; dislocation; periprosthetic fractures; extensor mechanism failure; non-specific prosthesis disruption; and prosthesis related infection (figure: rotating hinge implant failure; figure: periprosthetic fracture; figure: knee particle disease; figure: failure of bilateral knee arthroplasty; figure: patellar button dislocation) (Mulcahy, 2014).
Femoral-sided
lesions are often underestimated, because the
femoral component makes visualization of the
lesions difficult. Change in position of components
on serial images is indicative of prosthesis
loosening. Cross-sectional imaging and nuclear medicine imaging are often used along with standard radiography to evaluate joint arthroplasties for loosening, infection, and particle disease. Perfect radiographic views parallel to the bone-prosthesis interface are paramount.
Back to Top
Total ankle arthroplasty (TAA) or total ankle replacement (TAR) is rare, because ankle arthrodesis achieves excellent results with reduction of patient discomfort and good patient satisfaction (Easley, 2002). Despite the relatively increased forces on the ankle compared to the knee and the hip, the prevalence of symptomatic arthritis at the ankle is considerably less than that at the knee or the hip. Total knee arthroplasty (TKA) is performed 24 times more frequently than ankle arthrodesis or ankle arthroplasty combined (Yu, 2014).
The first generation of total ankle prostheses introduced in the 1970's had unacceptably high complication rates (figure: old generationTAR with settling) (Berquist, 1995; Freiberg, 2001). Implant designs for ankle arthroplasty have evolved considerably from constrained to less constrained and now have two or three component mobile bearing designs. Increased awareness of the ankle dynamics and better surgical training have made ankle replacement more successful and a promising alternative to ankle arthrodesis.
Appropriate patient selection remains a necessary first step for successful ankle replacement (Gougoulias, 2009). Total ankle replacement for younger patients and those with a more active life style as well as severe ankle deformities still remains very challenging. It also remains to be seen if the motion attained after total ankle arthroplasty offers any protection against ipsilateral subtalar joint complex arthritis.
Arthrodesis and resection arthroplasties are the most common procedures in the foot for inflammatory arthropathy and common degenerative conditions. However, small joint arthroplasty in the foot with newer designs is being applied to a number of everyday conditions with good short-term results. Arthroplasty of the small joints of the foot was originally performed mainly in patients with rheumatoid arthritis in which the metatarsophalangeal joints were replaced with Silastic and polyethylene spacers, most commonly in the great toe (Taljanovic, 2003). Because there was a high rate of complications and failure of the Silastic implants with breakage, fragmentation, synovitis, and bone resorption from particle disease, these types of procedures with Silastic implants have somewhat fallen out of favor with orthopedic surgeons.
It remains to be seen if current prosthesis designs for the small joints of the foot are sufficiently robust with good enough long-term results to replace more traditional surgical approaches for hallux rigidus, such as arthrodesis. Chronic pain in a first metatarsophalangeal implant arthroplasty is usually due to implant failure or infection (figure: right large toe hemiarthroplasty). The best treatment for implant failure is usually arthrodesis. This may require structural bone grafting with a somewhat slower healing time (Greisberg, 2014). Specific joint arthroplasty implants do not seem to offer any advantage for the treatment of hallux valgus compared to the more commonly used surgical procedures such as re-alignment and soft tissue augmentation.
Back to Top
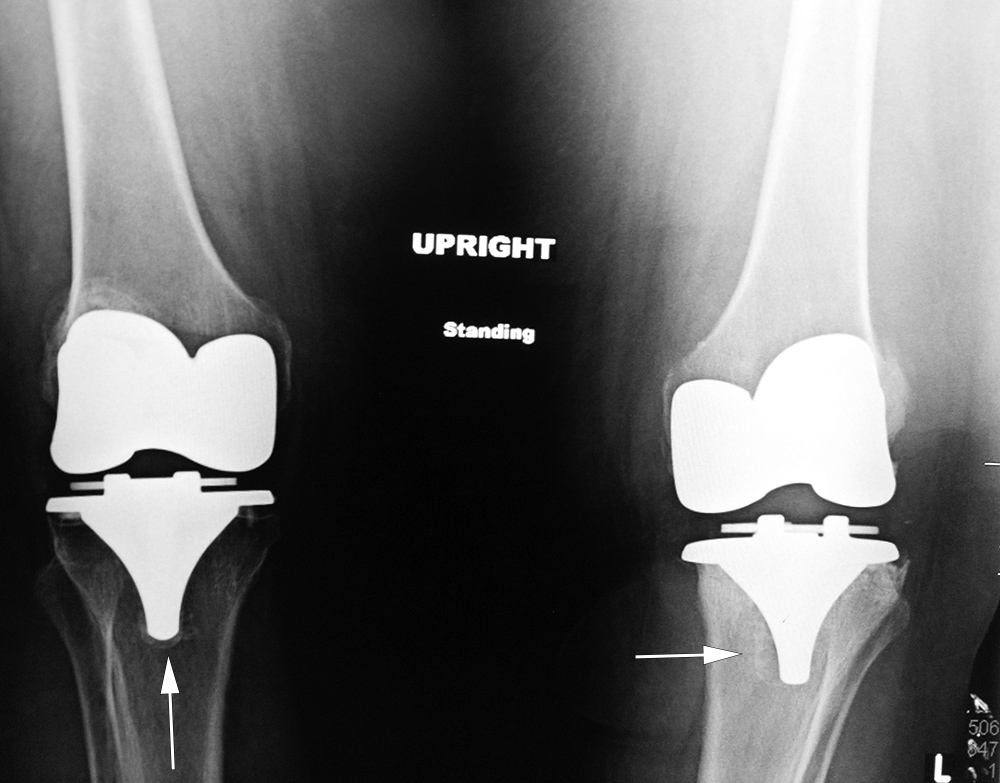
| Aseptic loosening of bilateral total knee arthroplasties |
 |
 |
 |
 |
| 65 year-old woman with bilateral cruciate-retaining total knee arthroplasties (TKAs) placed in early 2009. In November 2015 routine follow-up showed bilateral aseptic loosening in both tibial components with wide periprosthetic lucencies (arrows) and varus deformity on the left. From left to right, respectively, AP radiograph of the left knee in the postoperative period, AP radiograph of the left knee 6.5 years later, lateral radiograph of the left knee in the postoperative period, and lateral radiograph of the left knee 6.5 years later. Images courtesy Laura H Lee, MD. |
|
| Aseptic loosening of bilateral total knee arthroplasties continued |
 |
 |
 |
|
| 65 year-old woman with bilateral cruciate-retaining total knee arthroplasties (TKAs) placed in early 2009. In November 2015 routine follow-up showed bilateral aseptic loosening in both tibial components with wide periprosthetic lucencies (arrows) and varus deformity on the left. From left to right, respectively, AP radiograph of the right knee in the immediate postoperative period, AP radiograph of the right knee 6.5 years later, and standing frontal view of the knees 6.5 years after surgery. Images courtesy Laura H Lee, MD. |
|
| Rotating-hinge knee implant |
Rotating hinge knee implant failure |
 |
 |
 |
 |
| 69 year-old man with revision of an infected right knee prosthesis (two left panels). A rotating hinge knee implant was placed. Note the antibiotic beads about the medial aspect of the implant. The two fixation screws and wire are from prior surgery. There was implant failure with disruption of the implant six weeks later (two right panels). |
|
| Right total knee prosthesis patellar button dislocation |
Old generation total ankle arthroplasty with settling of tibial component |
Right ankle prosthesis failure with loosening of components and polyethylene wear medially |
 |
 |
 |
|
| The patellar component (button) is dislocated inferiorly (arrow) |
The tibial component has subsided into the distal tibia. There is significant surrounding radiolucency. From Benjamin, 1994. |
68 year-old woman with total ankle prosthesis failure with loosening of tibial and talar component shown by bony lucency about the components and medial polyethylene liner wearing. |
|
| Right large toe hemiarthroplasty |
|
|
|
 |
|
|
|
| 57 year-old woman with chronic pain at right large toe metatarsophalangeal joint. The hemiarthroplasty was later removed due to the development of hallux rigidus, and the joint was fused. From Taljanovic, 2003. Permission granted for use of images in this article by Radiological Society of North America (RSNA) |
|
|
|
Back to Top
|






















































{kind=link}