Orthopedic Devices
|
| |
|
|
|
|
|
|
Joint Arthroplasty - Ankle and Foot |
| |
|
|
|
|

|
Joint Arthroplasty - Ankle and Foot
by Tim B Hunter, MD, MSc
Ankle Arthroplasty
Total ankle arthroplasty (TAA) or total ankle replacement (TAR) is uncommon and reserved for end-stage ankle osteoarthritis and inflammatory arthropathy with the intent to preserve at least partial movement at the ankle joint. The main reason ankle arthroplasty is rare is that ankle arthrodesis achieves excellent results with reduction of patient discomfort and good patient satisfaction (Easley, 2002). The clinical outcome is good for ankle arthrodesis when fusion is obtained.
Potential disadvantages to ankle arthrodesis include malunion, nonunion, malalignment, limited range of motion, altered gait, and development of same side hindfoot joint arthritis requiring further surgery. Long-term follow-up shows many patients with tibiotalar arthrodesis have progressive symptomatic degenerative changes of the ipsilateral subtalar, talonavicular, and tarsometatarsal joints.
Even given the limitations for long-term success in ankle arthrodesis, ankle arthroplasty remains relatively rare, because the first generation of total ankle prostheses introduced in the 1970's had unacceptably high complication rates (figure: old generation TAR with settling) (Berquist, 1995; Freiberg, 2001; Omar, 2019).
Active infection locally at the ankle, systemic infection, significant peripheral
vascular disease, deficient soft tissues with poor wound healing as well as Charcot neuropathy are considered absolute contraindications for ankle arthroplasty. Relative contraindications
for total ankle arthroplasty are
young age, patients who are quite physically active, prior infection in the ankle or foot, severe
malalignment of the lower extremity, marked
ankle instability, significant osteoporosis, recent or evolving osteonecrosis
of the talus, and morbid obesity (Easley, 2002).
The ankle is a small joint through which all the body weight is supported. It is a complex hinge joint allowing both rotation and translation with a changing center of rotation. There are three articulations at the ankle: a) tibia with superior talar trochlea; b) fibula with lateral talus; and c) medial malleolus with medial talus. The talus has a changing axis of rotation moving from dorsiflexion to plantar flexion relative to the ankle mortise.
Compared to other weight-bearing joints of the lower extremity the ankle has significantly less contact area than the hip or knee. The knee is subjected to forces estimated to be 3 times the body weight, while the ankle is subjected to 5.5 times the body weight with normal ambulation (Yu, 2014). Despite the relatively increased forces on the ankle compared to the knee and the hip, the prevalence of symptomatic arthritis at the ankle is considerably less than that at the knee or the hip. Total knee arthroplasty (TKA) is performed 24 times more frequently than ankle arthrodesis or ankle arthroplasty combined (Yu, 2014).
Ankle trauma is the most common cause of degenerative changes at the ankle joint. Most ankle surgery is for end-stage ankle osteoarthritis resulting from the long term effect of prior or ongoing ankle trauma. Inflammatory arthropathies, particularly rheumatoid arthritis, are less common causes for end-stage ankle arthritis. On rare occasion hemochromatosis, infection, tumor, or neuropathic arthropathy affect the ankle joint to such a degree that surgery is required. Ankle arthropathy is frequent in hemophiliac patients, and ankle arthroplasty is a promising alternative to arthrodesis for hemophiliac patients (Asencio, 2014).
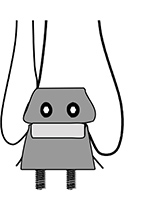
The first generation of total ankle prostheses introduced in the 1970's were highly constrained two part ball and socket design using cemented components (figure: old generation ankle implant). There was an all ultrahigh molecular weight (UHMWPE) polyethylene tibial component cemented into place. It articulated with a metallic talar component. These prostheses had unacceptably high failure rates and complications. Because of this, ankle arthroplasty was somewhat abandoned and ankle arthrodesis was used for end-stage ankle arthritis requiring surgery.
Arthrodesis is still the gold standard for treatment of end-stage ankle arthritis, but its limitations led to resurgence of interest in ankle arthroplasty. More modern total ankle replacement has excellent or good results in 82% of patients followed long term. Continued follow-up is necessary, but total ankle arthroplasty is a viable option for surgical treatment of ankle arthritis (Yu, 2014; Omar, 2019).
Implant designs for ankle arthroplasty have evolved considerably from constrained to less constrained and now have two or three component mobile bearing designs (figure 2nd and 3rd generation ankle arthroplasty; figure: semiconstrained Agility prosthesis; figure: third generation ankle prosthesis; figure: Zimmer trabecular metal ankle prosthesis).
More modern designs as approved and listed by the Aetna Insurance Clinical Policy Bulletin: Total Ankle Arthroplasty, number 06745 are the Scandinavian total ankle replacement
(STAR) [Small Bone Innovations, Inc], the INBONE Total Ankle (Wright Medical Technology), the Agility LP Total Ankle Replacement (DePuy Synthes), the Eclipse Total Ankle, the Salto Talaris Total Ankle Prosthesis (Tornier), and the Zimmer Trabecular Metal Total Ankle (Zimmer Holdings).
Several of these or similar designs are illustrated below (figure: STAR total ankle replacement; figure: Agility total ankle replacement; figure HINTEGRA total ankle replacement; figure Salto total ankle replacement; figure: INBONE II total ankle replacement; figure: Infinity Total Ankle System). Other systems are also available and approved by other insurance companies. Some products are widely available. Others are limited to Europe, the United States, or Japan.
The second generation of ankle prostheses are semiconstrained two component systems with a weight-bearing UHMWPE insert allowing sliding motion on one side of the insert. The polyethylene weight-bearing surface is either incorporated into the talar or the tibial component (figure: semiconstrained Agility prosthesis).
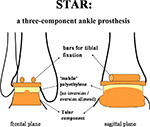
In the third generation of ankle prostheses there is a third component -- an independent polyethylene "meniscus". This allows for flexion and extension at the talar meniscal interface. Rotation and sliding takes place at the tibial meniscal interface (Yu, 2014). This design gives multiplanar motion and has improved joint congruency. It requires minimal bone resection. One disadvantage is the possible dislocation of the mobile meniscus and the need for tight implant fit to prevent instability (Yu, 2014). This design may also allow for more uneven polyethylene wearing leading to prosthesis failure (figure: ankle prosthesis failure).
To summarize, modern total ankle replacement (TAR) is classified as two component versus three component designs, sometimes respectively referred to as fixed-bearing, where the polyethylene meniscus is fixed to the tibial component, and mobile-bearing where the "meniscus" is free floating. One should realize, however, there is a confusing array of terms that are not necessary used consistently when describing more modern ankle arthroplasties.
The modern designs (second and third generation ankle prostheses) have abandoned cement fixation. They use improved metallic implant surfaces that induce bone overgrowth and reduce aseptic (non-infectious) loosening. The designs use different approaches for fixation into the tibia and talus, such as pegs, long stems, or short stems for tibial fixation, and cylindrical or rectangular bars for talus fixation and sometimes for tibial fixation as well.
Modern ankle prostheses are all porous coated for bone ingrowth. The components are made from a titanium alloy using a cobalt chrome polyethylene articulation. There is press fit insertion of the components, somewhat limited bone resection, and less constrained components compared to the earliest first generation TAR designs which used cemented, constrained components (Gougoulias, 2009; Yu, 2014). The two or three component designs allow for sliding, hinge, and rotational motions at the ankle.
In some TAR designs, such as the semiconstrained Agility prosthesis, syndesmotic fusion is used to prevent
tibial component subsidence (figure: Agility prosthesis). In most TAR designs there is resurfacing
of the medial and lateral ankle recesses to enhance
fixation and alignment. A
somewhat eccentric position of the talar component
within the tibial component is normal. This represents normal space
between the talar component and the polyethylene liner to allow more mobility of the ankle
prosthesis. A more marked eccentric position of the talar component or increasing asymmetry on follow-up radiographs should raise the question of prosthesis failure with abnormal polyethylene liner wearing and the development of particle disease (figure: right ankle prosthesis failure). The tibial component, whether it has a long rod configuration, a short rod configuration, or pegs for insertion into the tibia should have its articulating surface perpendicular to the long axis of the tibia (Taljanovic, 2003).
The length of the tibial fixation component stem varies considerably depending on the ankle prosthesis design. Those designs, such as the INBONE, have a relatively long tibial stem (figure: INBONE II ankle prosthesis). These are sometimes called an intramedullary-fixation total ankle arthroplasty. On relatively short-term follow-up (2-4 years) there are good patient reported outcomes and increased ankle motion with this type of TAR (Adams, 2014; Hsu, 2015). Others feel short pegs rather than long or short tibial stems are more useful, because bone strength at the distal tibia decreases rapidly with increasing distance from the tibial articular surface (Yu, 2014).
Complications from total ankle arthroplasty include neurovascular injury, tendon injury, and medial malleolar fracture in the intraoperative period. In the early postoperative period complications include medial malleolar stress fracture, distal fibular fracture, distal tibia fracture, hematoma or seroma formation, and infection with delayed wound healing. Aseptic loosening is the most common late postoperative complication. Excessive subsidence, periprosthetic fracture, expansile osteolysis, excessive spacer wear and migration, excessive heterotopic ossification, increased osteoarthritis in neighboring joints, and chronic regional pain syndrome as well as indolent infection are possible late postoperative complications (Bestic, 2008; Omar, 2019).
There are more complications from ankle arthroplasty than from ankle arthrodesis, but Increased awareness of the ankle dynamics and better surgical training have made ankle replacement more successful and a promising alternative to ankle arthrodesis. Annually, there are now about 10,000 total ankle replacements in the United States. Appropriate patient selection remains a necessary first step for successful ankle replacement (Gougoulias, 2009). It is possible for patients to successfully enjoy low impact recreational sporting activities, such as swimming, cycling, light fitness exercises, and weight training.
Total ankle replacement for younger patients and those with a more active life style as well as severe ankle deformities still remains very challenging. It also remains to be seen if the motion attained after total ankle arthroplasty offers any protection against ipsilateral subtalar joint complex arthritis. Subtalar joint arthritis if severe is usually treated by arthrodesis, though fixation screw stabilization is sometimes used (figure: subtalar joint interference screw).
Back to Top
| Old generation ankle implant |
Two and three component (second and third generation) ankle arthroplasty |
Scandinavian total ankle replacement
(STAR) |
Agility total ankle replacement |
 |
 |
 |
 |
| From Gougoulias, 2009 |
From Gougoulias, 2009 |
From Gougoulias, 2009 |
From Gougoulias, 2009 |
 |
| HINTEGRA total ankle replacement AP view |
HINTEGRA total ankle replacement lateral view |
SALTO total ankle replacement |
Old generation total ankle arthroplasty with settling of tibial component |
 |
 |
 |
 |
| This is a mobile-bearing three component ankle prosthesis |
From Gougoulias, 2009 |
The tibial component has subsided into the distal tibia. There is significant surrounding radiolucency. From Benjamin, 1994. |
|
| Semiconstrained Agility prosthesis-second generation ankle prosthesis |
Third generation total ankle arthroplasty (SALTO) |
Right ankle prosthesis failure with loosening of components and polyethylene wear medially |
 |
 |
 |
 |
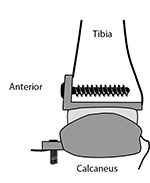
| Fixed bearing porous coated total ankle prosthesis with partially conforming articulation. There is a distal tibiofibular syndesmosis with two syndesmotic screws. Figure is from Taljanovic, 2003. |
There is also a subtalar joint arthrodesis stabilized by two large partially threaded cortical bone screws. |
68 year-old woman with total ankle prosthesis failure with loosening of tibial and talar components shown by bony lucency about the components and medial polyethylene liner wearing. |
|
| Zimmer trabecular metal total ankle prosthesis-3rd generation ankle prosthesis
|
Zimmer trabecular metal total ankle replacement-third generation ankle prosthesis |
 |
 |
 |
 |
| 67 year-old man with complex distal tibia and fibular fracture and delayed union in the tibia fracture. There are fracture fixation plates and screws in the tibia and fibula, suture anchors at the lateral malleolus, and a ghost track in the calcaneus. The ankle prosthesis was placed for treatment of severe osteoarthritis.
|
63 year-old woman with severe degenerative osteoarthritis. There is a fibular periarticular plate and screws for a fibular osteotomy. Ghost tracks are present in the calcaneus and tibia.
|
|
| INBONE II total ankle replacement |
Subtalar joint fusion with interference screw |
 |
 |
 |
 |
| |
|
69 year-old woman recovering from triple malleolar fracture with associated two medial malleolus fixation screws, two syndesmotic screws, and a fibular plate and screws. There is an interference screw in the subtarsal joint near the sinus tarsi from prior subtalar joint fusion. A fixation screw is present at the base of the 5th metatarsal from an old metatarsal shaft (Jones) fracture. |
|
| Infinity Total Ankle System (Wright Medical) |
Silastic (Swanson) great toe metatarsophalangeal joint arthroplasty |
|
|
 |
 |
|
|
| |
Patient with rheumatoid arthritis. The great toe arthroplasty was placed due erosive joint destruction at the great toe metatarsophalangeal joint. Note erosion of the 5th metatarsal head. |
|
|
|
| Smart Toe implants
|
Smart toe implant |
Right large toe hemiarthroplasty |
 |
 |
 |
 |
| 71 year-old woman with surgery for recurrent hammertoes. There are Smart Toe implants fusing the right second and third interphalangeal joints. A small cortical screw goes through the second metatarsal neck, and there are K wires in the fourth and fifth toes.
|
31 year-old woman with Smart Toe implant for fusion of the left second interphalangeal joint to correct painful hammertoe. |
57 year-old woman with chronic pain at right large toe metatarsophalangeal joint. The hemiarthroplasty was later removed due to the development of hallux rigidus, and the joint was fused. From Taljanovic, 2003 |
Back to Top
Foot Arthroplasty
Arthroplasty of the small joints of the foot is becoming more common. It was originally performed mainly in patients with rheumatoid arthritis in which the metatarsophalangeal joints were replaced with Silastic and polyethylene spacers, most commonly in the great toe (Taljanovic, 2003) (figure: great toe metatarsophalangeal joint Silastic (Swanson) arthroplasty). Because there was a high rate of complications and failure of the Silastic implants with breakage, fragmentation, synovitis, and bone resorption from particle disease, these types of procedures with Silastic implants are now rarely performed.
Arthrodesis and resection arthroplasties are the most common procedures in the foot for inflammatory arthropathy and common degenerative conditions. However, small joint arthroplasty in the foot with newer designs is being applied to a number of everyday conditions with good short-term results.
Bone destruction and deformities in the foot associated with rheumatoid arthritis often require surgical intervention. There are other more common foot conditions that require surgical consideration, because conservative measures are often ineffective in moderate to severe cases. These include hallux valgus, severe osteoarthritis at the great toe metatarsophalangeal joint (hallux rigidus), hammertoe and claw toe deformity, and a variety of deformities related to the soft tissue and bony destructive effects of diabetic neuropathy in the foot and ankle.
Hammertoe and claw toe deformity is very common in older adults and is sometimes disabling. A number of surgical approaches have been successfully used to treat these conditions including K-wire fixation, simple joint resection arthroplasty, proximal interphalangeal joint (PIP) arthrodesis with osteotomy, and interpositional implant arthroplasty (Sung, 2014; Kramer, 2015). Most of these techniques provide adequate pain relief and radiographic sagittal plane correction. The interpositional implant arthroplasty also provides significant radiographic correction in the axial plane (Sung, 2014). The significance of this observation is uncertain as there is sometimes poor correlation between radiographic findings and patient symptoms. The Smart Toe implant was designed for treatment of hammertoe deformity and is designed to facilitate joint arthrodesis (figure: Smart Toe implant).
Hallux rigidus is end-stage arthrodesis of the first metatarsophalangeal joint. Arthrodesis is the gold standard for the treatment of severe hallux rigidus. Treatment is now available to prolong the life of the joint or to mimic the biomechanics of the joint by replacing the entire joint with an arthroplasty or a portion of the joint with a hemiarthroplasty (figure: right large toe hemiarthroplasty).
In the short-term, metatarsal head resurfacing hemiarthroplasty for hallux rigidus provides good patient satisfaction and function (Erdil, 2012). However, a report by Titchner (2015) noted the revision rate for the TOEFIT-Plus (Smith & Nephew), which is designed for first metatarsophalangeal joint replacement for hallux rigidus, was unacceptably high in a mean follow-up of 33 months. The TOEFIT-Plus has a modular design allowing for its use as a hemiarthroplasty replacing only the first metatarsal head or as a full arthroplasty replacing the first metatarsal head and the proximal portion of the proximal phalanx of the first toe.
There were also mixed results for hemiarthroplasty of the proximal phalanx and distal oblique metatarsal osteotomy for hallux rigidus at 2 years follow-up (Ronconi, 2011). It remains to be seen if current prosthesis designs for the small joints of the foot are sufficiently robust with good enough long-term results to replace more traditional surgical approaches for hallux rigidus, such as arthrodesis.
Chronic pain in a first metatarsophalangeal implant arthroplasty is usually due to implant failure or infection. The best treatment for implant failure is usually arthrodesis. This may require structural bone grafting with a somewhat slower healing time (Greisberg, 2014).
Hallux valgus is the most common forefoot deformity. There are a number of common treatment options for hallux valgus and bunion formation. Surgical treatment is used after failure of more conservative methods. Nonoperative treatment can alleviate symptoms and may be all that is necessary. It does not correct the deformity of the big toe, however.
A distal first metatarsal osteotomy (Chevron osteotomy) is commonly used for severe hallux valgus, and if there is a severe deformity, there is also a proximal first metatarsal osteotomy as well as corrective soft tissue surgery. These osteotomies are usually stabilized by one or more fixation plates and screws. If there is associated osteoarthritis at the first metatarsophalangeal joint, a resection arthroplasty may be performed.
In patients who are physically quite active, an arthrodesis at the first metatarsophalangeal joint may be the best treatment option for hallux valgus (Wulker, 2012). Arthrodesis offers a better functional outcome compared to resection arthroplasty in patients with moderate to severe hallux valgus with degenerative changes at the first metatarsophalangeal joint (Little, 2014). Specific joint arthroplasty implants do not seem to offer any advantage for the treatment of hallux valgus compared to the more commonly used surgical procedures.
Back to Top
|


























{kind=link}