Joint Arthroplasty - Shoulder
by Tim B Hunter, MD, MSc
Shoulder Arthroplasty
Shoulder arthroplasty was first tried in 1893 by Jules-Emile Pean, a French surgeon who implanted a platinum and rubber prosthesis to replace a shoulder joint destroyed by tuberculosis (Schrumpf, 2011). The modern era for shoulder replacement began with the work of Charles Neer from 1951 to 1974 when the first modern total shoulder prosthesis, the Neer II was introduced. This consists of a metallic humeral head and stem component which articulates with a polyethylene glenoid resurfacing component. Since then, over 70 different shoulder prosthetic devices have been developed (Schrumpf, 2011).
The main indications for shoulder arthroplasty
are severe shoulder degenerative or inflammatory arthritis, humeral head osteonecrosis,
or a complex, highly comminuted proximal humerus/glenoid fossa fracture. More than 2/3 of shoulder arthroplasties are performed in patients older than 65 (Kim, 2011). In fact, shoulder arthroplasty is the third most common joint replacement after knee and hip replacement (Lin, 2016). The number of shoulder arthroplasties performed annually in the United States is increasing rapidly and is estimated to number between 55,000 and 80,000 (AAOS, 2016). This reflects the increased wear and tear shoulder arthritis in older patients, the increasing longevity of the population, and the increased success of shoulder joint replacement. It also reflects the growing number of surgical options for shoulder joint replacement or partial replacement.
There are several possible surgical options for complete or partial shoulder joint replacement: a) anatomic shoulder arthroplasty with complete replacement of the humeral head and glenoid fossa; b) reverse total shoulder arthroplasty with complete replacement of the shoulder joint; c) shoulder hemiarthroplasty with replacement of the humeral head; and d) humeral head resurfacing (Petscavage, 2012 Parts 1 and 2; Gustas-French, 2018). Total shoulder arthroplasties are somewhat more common than shoulder hemiarthroplasty or humeral head resurfacing. Kim (2011) and co-authors estimate in 2008 approximately 27,000 total shoulder arthroplasties and 20,000 hemiarthroplasties were performed. Reverse total arthroplasty was approved by the United States Food and Drug Administration (FDA) in 2003 and probably is part of the reason why there has been an increased incidence of shoulder arthroplasty in the United States in recent years (Kim, 2011).
Modern shoulder arthroplasty started with the pioneering work of Neer in 1955 (Walch, 2010; Neer, 1955). With an intact rotator cuff and an unconstrained prosthesis there is a prosthesis survival rate of 97% after 10 years and 84% after 20 years for total shoulder arthroplasty (TSA). For patients who have complex, comminuted proximal humerus fractures (3 or 4 part), how well the greater tuberosity heals determines the outcome of the shoulder arthroplasty (Walch, 2010).
The long term results for other forms of shoulder joint replacement (shoulder hemiarthroplasty, reverse total shoulder arthroplasty, humeral head resurfacing) are somewhat less impressive but are improving. They are good enough though to provide a variety of shoulder joint surgical options for patients with severe proximal humerus fractures, massive rotator cuff tears, and surgical or bony destruction from tumor or infection, or for patients needing revision of a failed prior shoulder arthroplasty.
Anatomic Shoulder Arthroplasty
The prosthetic humeral head component
is anchored in the proximal humerus in an anatomic shoulder arthroplasty or hemiarthroplasty. Total shoulder arthroplasty (TSA), also known as total shoulder replacement (TSR) requires an intact functioning rotator cuff for the best success. A modular metallic humeral head with a metallic stem articulates with the native
glenoid in a shoulder hemiarthroplasty or
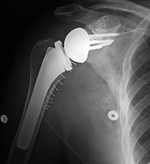
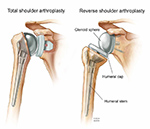
with a prosthetic glenoid component in a shoulder arthroplasty (figure: drawing of total shoulder arthroplasty and reverse total shoulder arthroplasty; figure: right shoulder hemiarthroplasty; figure: right total shoulder arthroplasty). The glenoid component may be metal backed and secured by screws or composed of polyethylene and cemented into place. Polyethylene glenoid components have one or more metallic pegs or indwelling wires to make them radiographically visible.
The majority of humeral components have successful long term fixation without bone cement. For the glenoid component, many consider cemented all-polyethylene glenoid components to be the standard for anatomic shoulder arthroplasty (Sanchez-Sotelo, 2011; Gustas-French, 2018). Two
general types of the glenoid components are used:
keeled (polyethylene with an indwelling wire
loop) and pegged (metal).
The type of total shoulder prosthesis used
depends on patient selection, the surgeon’s preference,
and the surgeon’s experience (Sanchez-Sotelo, 2011). Shoulder
prostheses are much less constrained than hip
prostheses. Shoulder prosthesis functionality depends to a
great degree on competency of the rotator cuff.
The Total Evolutive Shoulder System (TESS, Biomet) and the Affinis (Mathys) are arthroplasty designs that do not use the traditional long metal stem for the humeral component (figure: TESS prosthesis). There is less bone removal and possible less soft tissue disruption. The humeral head can be positioned despite any deformity of the humeral diaphysis, making these prostheses potentially most useful in patients with post-traumatic osteoarthritis of the shoulder and deformity in the proximal metaphysis of the humerus (Berth, 2013). There is also more humeral bone stock should revision surgery become necessary. While the mid-term results are good for this type of design, further investigation is necessary to determine the long-term performance of these prostheses, because the long-term results for the more traditional designs are good.
Foreshortening of the humeral neck
commonly occurs following proximal humeral
fractures. In all cases, it should be avoided during the placement of a shoulder prosthesis, since it compromises
the function of the shoulder (Lazarus, 2002; Boileau, 2002; Boileau, 2006). Shoulder arthroplasty is usually a very successful procedure with good pain relief and improvement in shoulder motion and function.
The initial postoperative radiographs frequently show thin radiolucent areas about the prosthesis, particularly
about the cemented glenoid component. In most cases they are likely related to difficulty in achieving good
cement penetration into the bone and are of no consequence. However, on subsequent
radiographs there should be no progression of any radiolucent lines at the implant-
bone interfaces, since they may indicate loosening and/or infection.
Loosening can occur about either the humeral or glenoid component
(Lazarus, 2002; Boileau, 2002; Boileau, 2006). At first, it may be difficult to differentiate prosthesis loosening unrelated to infection versus an infection related surgical complication.
The main complications seen with shoulder
arthroplasty are loosening and subluxation or dislocation.
Periprosthetic humeral shaft fractures
can occur intra-operatively or after surgery secondary
to trauma (Lazarus, 2002; Boileau, 2002; Boileau, 2006) (figure: right shoulder prosthesis periprosthetic fracture).
Back to Top
Shoulder Hemiarthroplasty
Shoulder hemiarthroplasty is a less invasive procedure with somewhat less bony and soft tissue disruption than total shoulder arthroplasty. The glenoid portion of the shoulder joint is left intact. Shoulder hemiarthroplasty is preferred over a total shoulder arthroplasty if the glenoid is relatively
normal. This is often true with comminuted proximal humerus fractures. It is often the case in humeral head osteonecrosis and in some cases of less severe osteoarthritis and rheumatoid arthritis. Shoulder hemiarthroplasty is occasionally used as part of the repair for severe rotator cuff tears. Shoulder hemiarthroplasty is also indicated where there is not enough bone stock to support a prosthetic glenoid component and a total shoulder arthroplasty.
Shoulder hemiarthroplasty is generally not indicated in cases of moderate to severe shoulder osteoarthritis. Total shoulder arthroplasty (TSA) is superior to shoulder hemiarthroplasty in these cases. TSA gives better pain relief, active range of motion, and patient satisfaction with similar complication rates (Boileau, 2006; Radnay, 2007). Shoulder hemiarthroplasties performed for osteoarthritis gradually deteriorate from erosion of the native glenoid. There is a significant increased rate of revision surgery with shoulder hemiarthroplasty compared with total shoulder arthroplasty (Radnay, 2007).
The humeral component of a shoulder hemiarthroplasty is often the same as the humeral component of an anatomic total shoulder arthroplasty. It articulates directly with the native glenoid fossa and can be cemented
or and press fit (interference fit) into place. In cases where there is a rotator cuff tear the prosthetic humeral head is somewhat laterally extended. This helps prevent bony impingement between the greater tuberosity of the humerus and the acromion (Petscavage, 2012 Part 1).
The hemiarthroplasty design may be used for upper extremity limb sparing prostheses where the prosthetic humeral head directly articulates with the glenoid fossa, and the humeral limb of the prosthesis is extended replacing all of part of the humerus after widespread surgery for a malignant tumor (figure: upper extremity limb sparing prosthesis).
There are multiple complications associated with shoulder joint hemiarthroplasty, similar to other arthroplasties, including prosthesis dislodgement, infection, and periprosthetic fracture. Specific complications to look for with shoulder hemiarthroplasty include progressive erosion of the glenoid fossa, partial or complete tearing of the rotator cuff with elevation of the prosthetic humeral in respect to the glenoid and acromion, and dislocation of the prosthetic humeral head out of the glenoid fossa (Gustas-French, 2018) (figure: hemiarthroplasty anterior dislocation).
Back to Top
Reverse total shoulder Arthroplasty
Full thickness rotator cuff tear is a common chronic ailment in older adults. There is associated superior migration of the humeral head, unopposed deltoid contraction, and ineffectiveness of the glenohumeral fulcrum mechanism. This causes one to lose the ability to raise the arm above the horizontal, so called shoulder "pseudoparalysis" (Ha, 2012; Roberts, 2007). There is associated secondary shoulder arthropathy and pain.
The prime indication for reverse total shoulder arthroplasty (RTSA or RSA) is a full thickness rotator cuff tear. RTSA is sometimes used for acute three or four part proximal humerus fractures, shoulder reconstruction after tumor surgery, and shoulder revision arthroplasty (Walch, 2010; Gustas-French, 2018). An intact deltoid muscle is needed for reverse total shoulder arthroplasty (Lin, 2016).
The reverse approach to shoulder arthroplasty was introduced by the French surgeon Paul M Grammont and approved in the United States in 2004 (AAOS, 2016). About half of the arthroplasties now being performed use the reverse design.
Reverse total shoulder arthroplasty reverses the ball and socket relationship of the shoulder joint, the prosthetic glenoid component being a ball and the humeral component a socket (Roberts, 2007) (figure: reverse shoulder arthroplasty). Since the joint center is moved distally and medially, there is more control of the shoulder joint motion by the deltoid muscle. This helps overcome the large motion loss from the deficit of the rotator cuff. Active elevation can be restored in patients with an irreparable rotator cuff tear or severe arthritis, but internal and external rotation of the shoulder is limited (Boileau, 2006).
The typical RSA has a cupped humeral component attached to a metal stem. Its radiolucent polyethylene liner sits in the cup and articulates with the metallic head (glenosphere) attaching to a base plate (metaglene) in the glenoid. The base plate is attached to the glenoid by bicortical screws (Roberts, 2007). The glenosphere should be aligned fully within the humeral cup, though the separation between the glenosphere and the humeral cup depends on the thickness of the polyethylene liner (figure: left shoulder reverse total shoulder arthroplasty).
The most common complication for a reverse total shoulder arthroplasty is anterior dislocation which often occurs in the early postoperative period (Ha, 2012). In this case, the humerus with its prosthetic cup lies anterior and superior to the glenosphere. This is due to the pull of the deltoid muscle. Posterior dislocation can also occur (figure: posterior dislocation in a RSA). Either anterior or posterior dislocation may be difficult to appreciate on standard frontal views due to the variable normal distance between the humeral cup and glenosphere depending on the thickness of the polyethylene liner. Any suspected dislocation has to be confirmed on orthogonal views, the axillary view if obtainable being the most reliable.
Scapular notching is very common after reverse total shoulder arthroplasty with bone resorption of the inferior scapular border (Lin, 2016) (figure: left shoulder reverse total shoulder arthroplasty). This probably results from change in the shoulder's center of rotation with repetitive contact between the humeral cup of the reverse total shoulder arthroplasty and the inferior scapular border. The importance of the bone resorption is uncertain. In minor cases it is probably best watched, while advanced grades of scapular notching, grades 3 and 4 on the Sirveaux classification scale (see below) may indicate additional surgery (Lin, 2016). Scapular spine and acromion fractures are also found with reverse shoulder arthroplasty in a small per cent of patients and may be a risk for prosthesis displacement in more severe cases. Radiographic evaluation of a reverse shoulder arthroplasty should include searching for scapular notching and subtle scapular spine or acromion fractures.
Sirveaux Scapular Notching Scale (adapted from Sirveaux, 2004).
Grade 1 - defect within the inferior pillar of the scapular neck; Grade 2 - erosion of the scapular neck to the level of the inferior fixation screw of the glenosphere; Grade 3 - extension of the erosion to over the lower fixation screw; Grade 4 - extension of erosion to the undersurface of the glenosphere base plate.
Back to Top
Humeral Head Resurfacing
Humeral head resurfacing replaces the humeral joint surface with a metallic covering or metal cap. It preserves the bone of the proximal humerus. Humeral head resurfacing was developed for younger patients and for those with primary humeral head abnormalities, such as avascular necrosis or localized humeral head articular cartilage loss (Gustas-French, 2018; Chen , 2019). The glenoid may be replaced with a polyethylene glenoid replacement but is often left intact with the humeral metal cup positioned flush against the glenoid surface. Since no humeral osteotomy has been performed, the head-shaft angular relationship of the humerus does not have to be addressed. There is minimum bone resection compared to the other forms of shoulder arthroplasty minimizing the operative time. There is also a low prevalence of periprosthetic fractures and further surgery for revision arthroplasty is somewhat easier (Burgess, 2009). Another advantage to this procedure is fewer metallic related artifacts on subsequent CT or MRI studies of the shoulder (Petscavage, 2012).
Often a Copland shoulder prosthesis is used for humeral head resurfacing. The Copland prosthesis consists of a metal cup that fits over the resected area of the humeral head. The cup has a metal peg for cementless insertion into the proximal humeral shaft. A similar design uses a threaded screw instead of peg to insert into the humeral shaft (figure: left shoulder resurfacing hemiarthroplasty). An occasional use for such a prosthesis is to cover a Hill-Sachs or reverse Hill-Sachs deformity (figure: left humeral head hemi-cap).
The long term outcome of humeral head resurfacing compared to the other forms of shoulder arthroplasty has yet to be determined. Since humeral head resurfacing produces less bony and soft tissue disruption, it has potential for better long term results and is a particular option for shoulder replacement in younger patients. Partial humeral head resurfacing may have an especial application for patients with advanced osteonecrosis of the humeral head (Uribe, 2009). It may also have application in some patients with rheumatoid arthritis affecting the shoulder joint, but it is not suitable for severely damaged joints, particularly if the humeral head is soft or has insufficient bone (Levy, 2004).
The metallic humeral head cup should be flush against the articular surface of the glenoid and not displaced anteriorly or posteriorly on axillary or scapular Y views. There should be minimal lucency about the metallic peg or screw which inserts into the humeral shaft (Petscavage, 2012 Part I).
Back to Top
Limb salvage (limb sparing) surgery (LSS) has greatly improved the comfort and quality of life for patients with devastating tumors or injuries involving the upper and lower extremities. Two decades ago, a malignant bone or soft tissue sarcoma meant a large amputation. The risk of leaving any portion of the tumor behind led to widespread resection, and there were poor means for reconstructing the limb (Cleveland Clinic).
Due to advances in chemotherapy, radiation therapy, and tumor surgery, as well as development of orthopedic appliances for upper and lower limb salvage, there has been a significant reduction in amputations for limb neoplasms. Neo-adjuvant therapy with chemotherapy and/or radiation therapy often shrinks tumors making them easier to remove. The surgeon can save considerable tissue and key structures such as major bones, nerves, and blood vessels.
Robotic extremities are now reaching a level of sophistication in which both sensory and motor components can be included in the prosthesis so it functions similar to a normal limb. There is an experimental implant which permits bidirectional communication between a prosthetic hand and electrodes implanted in the nerves and muscles of the remaining portion of a transhumeral amputation (Ortiz-Catalan, 2020). The prosthesis is a bone anchored robotic arm secured to the upper portion of the humerus by osseointegration. The long term success of such robotic arms remains to be determined, but such prostheses no doubt will be increasingly introduced for both the upper and lower extremities.
Back to Top
| Right shoulder hemiarthroplasty |
Total shoulder prosthesis (arthroplasty) |
Right total shoulder arthroplasty |
Right total shoulder arthroplasty |
 |
 |
 |
 |
| From Taljanovic, 2005 |
From Benjamin, 1994 |
The glenoid component is cemented in place and the humeral component is press fit. |
|
 |
| Right shoulder hemiarthroplasty |
Left shoulder reverse total shoulder arthroplasty |
 |
 |
 |
 |
| 61 year-old woman with bilateral shoulder prostheses. On the right there is a hemiarthroplasty. Notice the suture holes by the neck of the prosthesis for reconstructing the rotator cuff. On the left there is a reverse total shoulder arthroplasty. There is possible impingement on the inferior glenoid rim with beginning bone loss, "scapular notching" (arrow). |
|
| Left shoulder resurfacing hemiarthroplasty |
Limb sparing prosthesis (hemiarthroplasty) |
Left shoulder hemiarthroplasty anterior dislocation |
 |
 |
 |
 |
| Skin staples are also present |
This prosthesis was placed to spare the left upper extremity after widespread surgery for a metastatic bone tumor. The native glenoid is intact and articulates with the prosthetic humeral head. |
|
|
|
| Reverse total shoulder replacement arthroplasty plus skin staples |
Posterior dislocation of a reverse total shoulder arthroplasty
|
Right shoulder prosthesis periprosthetic fracture |
 |
 |
 |
 |
| This is particularly used for patients with rotator cuff arthropathy. |
|
|
51 year-old woman |
|
| Left shoulder humeral head Hemi-CAP |
Anatomic Drawing of total shoulder arthroplasty and reverse total shoulder arthroplasty |
TESS shoulder replacement system |
 |
 |
 |
 |
| 46 year-old man with left humeral head hemi-cap from treatment of chronic reverse Hill-Sachs deformity. Heterotopic bone is forming about the shoulder joint. |
Used with permission of Mayo Foundation for Medical Education and Research, all rights reserved. |
(From Bone and Joint Specialists, Waterford, MI) |
|
| Left Shoulder humeral head Hemi-CAP |
|
|
 |
 |
|
|
| 48 year-old man with multiple left shoulder dislocations. |
|
|
Back to Top
|





















