|
|

|
Joint Arthroplasty - Knee continued
by Tim B Hunter, MD, MSc
Unicompartmental Knee Arthroplasty; Knee Hemiarthroplasty (Interpositional Arthroplasty)
Isolated medial or lateral compartment knee osteoarthritis is sometimes treated by unicompartmental (unicondylar) knee arthroplasty (UKA). Unicompartmental osteoarthritis of the knee is not uncommon occurring in up to 40% of patients (Berend, 2015). Osteoarthritis isolated to the medial compartment is the most common. Therefore, most unicompartmental knee arthroplasty is performed in the medial compartment with prosthetic replacement of the medial femoral condyle and the medial tibial plateau. In fact, medial unicompartmental knee replacement is 10 times more common than lateral unicompartmental knee replacement (figure: medial unicompartmental knee arthroplasty; figure: lateral unicompartmental knee arthroplasty). Patellofemoral unicompartmental arthroplasty can also be performed, though it is rare compared to other forms of unicompartmental arthroplasty.
Unicompartmental knee arthroplasty was originally introduced in the 1970's but mainly abandoned until recently due to the poor survival of the prosthesis with high revision rates. It does lend itself to minimally invasive surgical techniques, and more modern prosthesis designs coupled with meticulous surgical techniques have made unicompartmental knee arthroplasty again popular (Riff, 2014). There is resurfacing of both sides of a single articular compartment of the knee joint. The prosthesis typically consist of a metallic femoral component and a metallic tibial component with a polyethylene articular weight-bearing surface.
High tibial osteotomy (HTO) can delay the need for total knee arthroplasty and may be chosen by younger patients who prefer joint preserving surgery. It is for patients seeking treatment of medial knee compartment osteoarthritis. The best patients for this are young, non obese, active individuals with varus deformity (Li, 2022; Rodrigues, 2022).
The risk of prosthesis failure and revision following a unicompartmental arthroplasty remains greater than that with primary total knee arthroplasty. The most common indications for revision are aseptic (non-infectious) prosthesis loosening and progression of osteoarthritis. The outcomes following revision for a failed unicompartmental knee arthroplasty are poorer than those following a successful unicompartmental arthroplasty or a successful primary total knee arthroplasty. In one series 5.3% of medial unicompartmental knee arthroplasties were revised at a mean of 25 months (Craik, 2014). In another series the mid-term (up to 8 years) outcomes for medial unicompartmental knee arthroplasty were excellent, but there was a high 9.8% incidence of complications (Ji, 2014).
In selected patients, sometimes the very young or the very old, unicompartmental knee replacement is a reasonable alternative to total knee arthroplasty. However, unicompartmental knee arthroplasty requires very careful selection of patients and meticulous surgical technique (Riff, 2014). The higher revision/re-operation rate for unicompartmental arthroplasty has to be balanced against its lower occurrence of complications, readmission, and mortality compared to total knee arthroplasty (Liddle, 2014).
Knee hemiarthroplasty (interpositional arthroplasty) is rare compared to unicompartmental knee arthroplasty or total knee arthroplasty. It is also rare compared to hemiarthroplasty in the shoulder or hip. In most cases knee hemiarthroplasty deals with osteoarthritis in the medial compartment of the knee joint. A knee spacer implant, either composed of biologic material, metal, or PEEK is placed in the medial compartment of the joint (figure: left knee joint interpositional arthroplasty). This is designed to address bone-on-bone apposition in the joint from the loss of the normal joint cartilage. The biologic spacer consists of an allograft meniscus, while the metal spacers are composed of cobalt-chrome alloy. PEEK spacers may be superior to biologic and cobalt-chrome alloy spacers, because PEEK spacers are more compliant to the femoral condyle reducing early postoperative pain. No matter the design, the spacers rest on the tibial plateau. There are no moving parts or cement fixation. The spacers are held in place by their close fitting shape to the tibial plateau.
The knee hemiarthroplasty has the advantage of requiring no bone cuts or component fixation. Its indication is medial compartment osteoarthritis of the knee where a unicompartmental arthroplasty and/or high tibial osteotomy would be performed. Unfortunately, the clinical results for knee hemiarthroplasty have been disappointing with a high rate of revision surgery. It also provides unpredictable pain relief (Baillie, 2008). Knee hemiarthroplasty may be a reasonable surgical option for patients who cannot have a corrective tibial osteotomy or who may be too young and too active for a unicompartmental or total knee arthroplasty (Springer, 2006). Nevertheless, it is an uncommon procedure and not often seen in routine orthopedic or radiologic practice.
Back to Top
Knee Arthroplasty: Complications
Knee replacement surgery is quite successful with good long term results for most patients. Since many of the patients for joint replacement surgery are predominantly older, there is a low but noticeable mortality and postoperative morbidity (Mulcahy, 2014). In one study (Pedersen, 2014) the risk of venous thromboembolism in patients treated with thromboprophylaxis is approximately 1.3% within 90 days of total hip replacement (THR) or total knee replacement (TKR) surgery with an annual risk between 0.9% and 1.6% for thromboembolism and between 0.4% and 0.8% for bleeding in patients followed 15 years. The risk of a patient dying within 90 days decreased from 1% in 1997 to 0.6% in 2011. The risk of stroke or myocardial infarction was 0.5% within 90 days of surgery. Patients in routine clinical practice in this study had a combined 3% risk of venous thromboembolism, myocardial infarction, stroke, or bleeding withing in 90 days of having total hip replacement or total knee replacement surgery (Pedersen, 2014).
The 45-day mortality after knee replacement surgery for osteoarthritis in England and Wales showed a decrease in mortality from 0.37% in 2003 to 0.20% in 2011. Unicompartmental knee replacement was associated with substantially lower mortality than total knee replacement (Hunt, 2014). Older patients have common co-morbidities of myocardial infarction, cerebrovascular disease, renal disease, and moderate to severe liver disease which increases operative mortality and postoperative morbidity. High levels of co-morbidities and general anesthesia are risk factors for venous thromboembolism and bleeding with no differences between THR and TKR surgeries (Pedersen, 2014).
Even nonagenarians (patients aged 90 and over) may be candidates for total knee arthroplasty. They do have a greater number of co-morbidities preoperatively with a higher rate of postoperative deep vein thrombosis, a longer hospital stay, and increased 30 day mortality (Mirac, 2014).
The effort to reduce mortality in the large study from England and Wales (Hunt, 2014) suggested concentrating efforts on older patients, particularly males. The co-morbidities especially have to be adequately addressed prior to surgery. For example, patient with cirrhosis who undergo total hip arthroplasty or total knee arthroplasty have significantly increased risk of medical complications, surgical complications, and death. Patients with a MELD (Model for End-Stage Liver Disease) score of 10 or greater have a three times increased likelihood of any complication and a 4.1 times increased likelihood of death within 90 days of the procedure (Tiberi, 2014). In almost all studies the mortality and morbidity rates appear to be consistently higher for men than women (Mulcahy, 2014).
Many of the immediate postoperative complications are systemic and often related to known co-morbidities rather than complications related to the knee surgery itself. Hematoma or seroma formation is the most common immediate postoperative complication related to the knee arthroplasty surgery. In almost all cases of orthopedic surgery in which the bone marrow is disturbed there is systemic fat embolism with emboli going to the lungs. Fortunately, this rarely produces fat embolism syndrome which is uncommon but occurs most often after traumatic bone fracture (Dhar, 2012; Tsai, 2010).
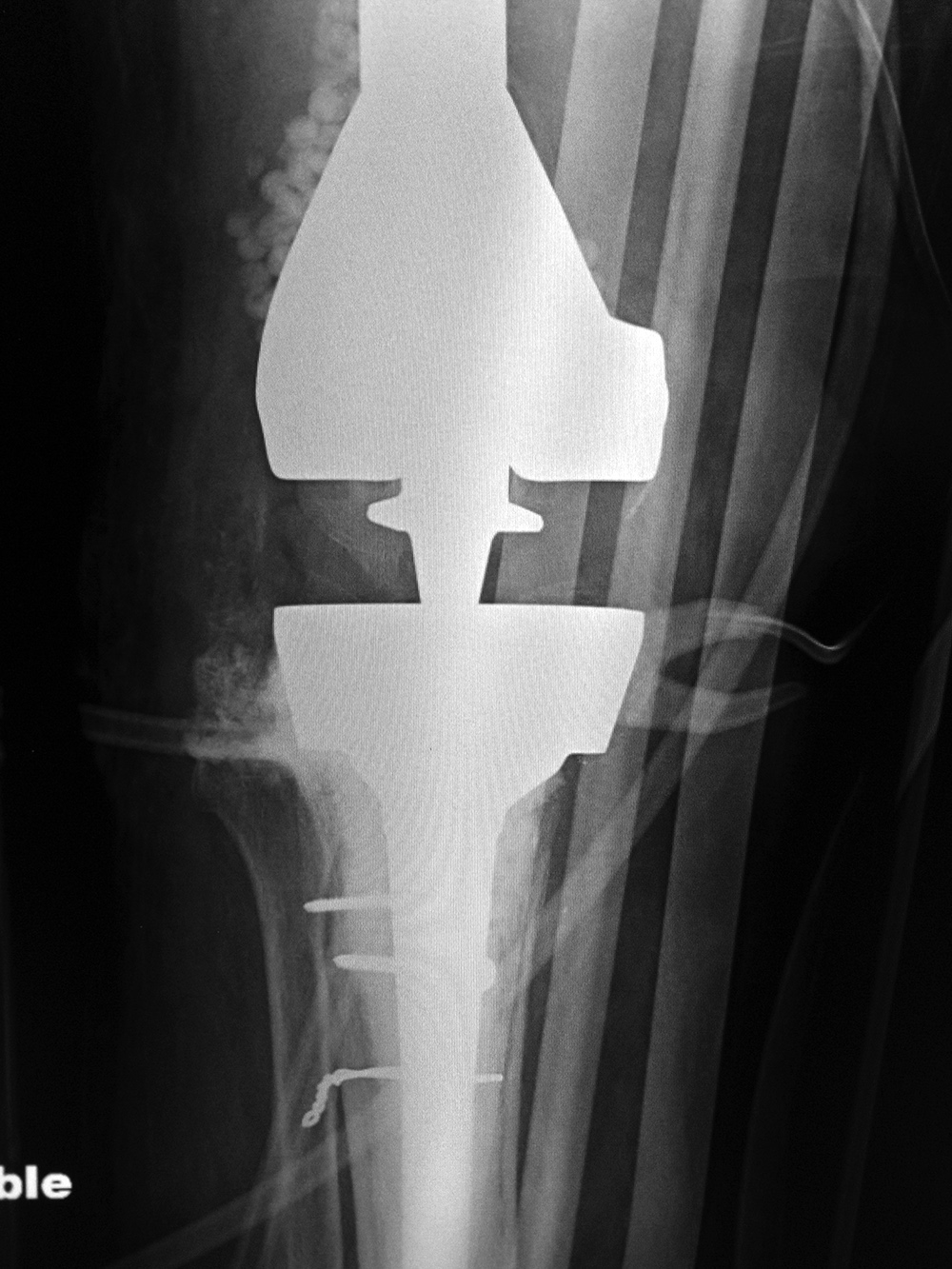
Long term complications associated with knee arthroplasty are similar to those seen with hip arthroplasty. They include include non-infectious aseptic
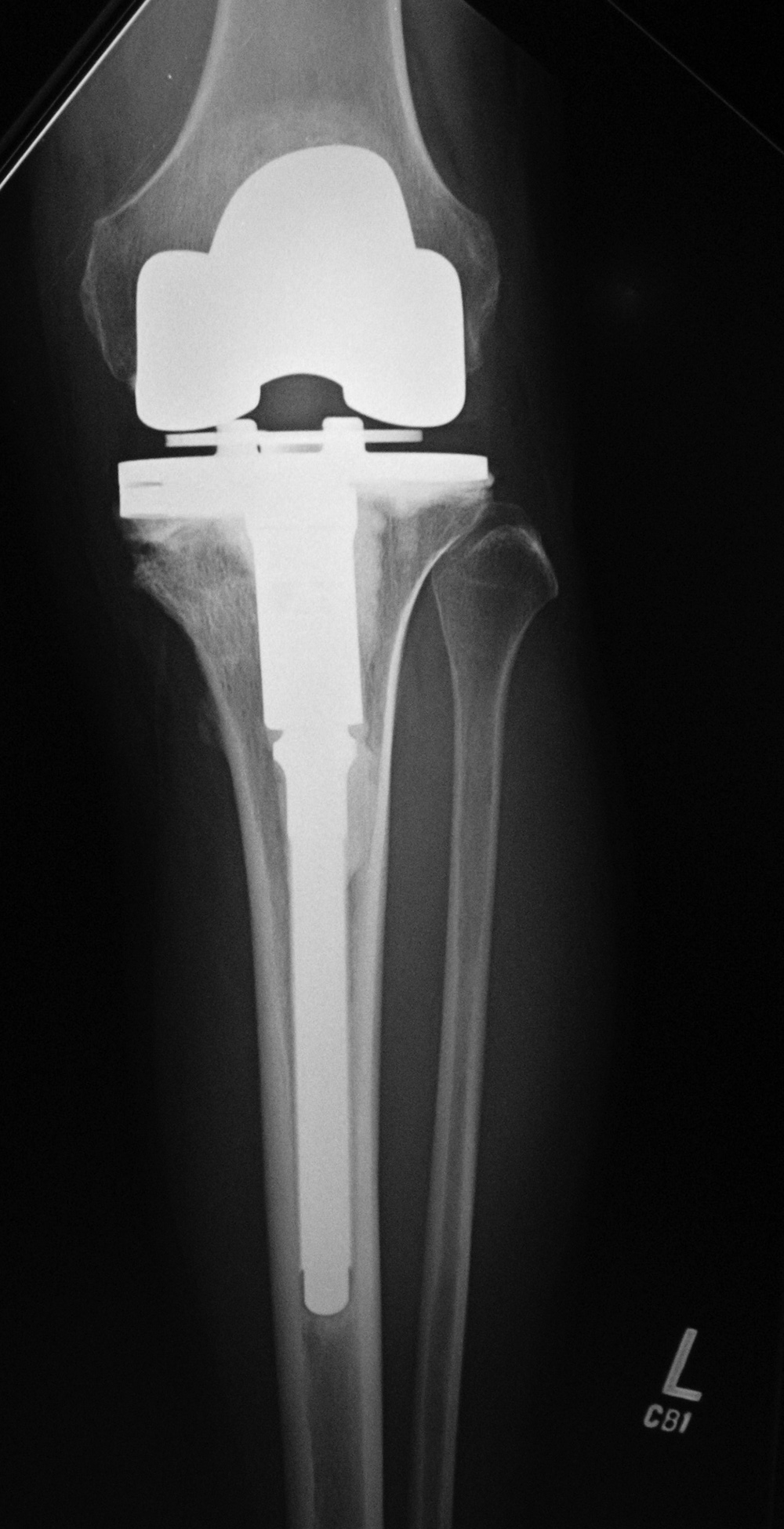
loosening from a varying combination of polyethylene wear, small particle disease, or non-specific osteolysis; periprosthetic fractures; extensor mechanism failure; non-specific prosthesis disruption; and prosthesis related infection (figure: rotating hinge implant failure; figure: periprosthetic fracture; figure: disrupted knee prosthesis; figure: knee particle disease; figure: failure of bilateral knee arthroplasty) (Mulcahy, 2014).
Stiffness after total knee arthroplasty is common and adversely affects long term outcome and patient satisfaction. A reduced preoperative range of motion, history of prior knee surgery, incorrect positioning or improperly sized components may be factors in some cases. Infection, arthrofibrosis, regional pain syndrome, and heterotopic bone formation may also be factors and should be considered in the workup for stiffness. Even so, stiffness after TKA is challenging as the cause is often not apparent or easily treatable. Conservative therapy after eliminating obvious causes (infection, malpositioned components) is the first step to be taken. This includes physical therapy and possible knee manipulation under anesthesia. At times, surgical lysis of adhesions may be necessary. If there is an obvious surgical error with component malpositioning, revision arthroplasty is indicated (Manrique, 2015).
Thin radiolucent
lines are seen commonly under the tibial component of a total knee arthroplasty but may be hidden by the metal tray if the
view is not perfectly tangential to the component
surface. Non-progressive radiolucent lines or areas less than 2 mm in
size are usually considered benign and incidental. On the other hand, progressive, circumferential,
radiolucent areas larger than 2 mm are usually viewed as indicating prosthesis loosening, which is most often on an aseptic basis (figure: failure of bilateral knee arthroplasty). Any findings suggestive of prosthesis loosening must include deep periprosthetic infection as a consideration. While not common, a noncemented tibial component may show failure by subsidence or settling of the anterior portion of the tibial tray into the metaphyseal bone (figure: subtle TKA failure).
Many orthopedic surgeons believe that polyethylene
wear (particle disease), which is often asymmetric, can best be appreciated
on weight-bearing views. Others think
that osteolysis is present long before there is enough
wear to decrease the joint space. Osteolytic lesions
occur in both the tibia and femur. A �
system similar to that for hip arthroplasty proximal femoral
stem components is used to divide and evaluate
the tibial component–bone interface into
zones 1–7. Tibial component failure is more common
than femoral component failure.
Femoral
lesions are often underestimated, because the
femoral component makes visualization of the
lesions difficult. Change in position of components
on serial images is indicative of prosthesis
loosening. Cross-sectional imaging and nuclear medicine imaging are often used along with standard radiography to evaluate joint arthroplasties for loosening, infection, and particle disease.
In general, dramatic pain relief is associated with total knee replacement. It is usually preferable to conservative therapy in patients with knee osteoarthritis who are eligible for total knee replacement; nevertheless, there is a small but not inconsequential increase in serious adverse events for patients treated with knee arthroplasty versus nonsurgical treatment (Skou, 2015; Katz, 2015).
Back to Top
Limb salvage surgery
Limb salvage (limb sparing) surgery (LSS) has greatly improved the comfort and quality of life for patients with devastating tumors or injuries involving the upper and lower extremities. Two decades ago, a malignant bone or soft tissue sarcoma meant a large amputation. The risk of leaving any portion of the tumor behind led to widespread resection, and there were poor means for reconstructing the limb (Cleveland Clinic).
Due to advances in chemotherapy, radiation therapy, and tumor surgery, as well as development of orthopedic appliances for upper and lower limb salvage, there has been a significant reduction in amputations for limb neoplasms. Neo-adjuvant therapy with chemotherapy and/or radiation therapy often shrinks tumors making them easier to remove. The surgeon can save considerable tissue and key structures such as major bones, nerves, and blood vessels.
The Cleveland Clinic reports that 60-65% of patients with osteosarcoma can be cured without amputation (Cleveland Clinic). Elbow prostheses probably provide better upper extremity function for treatment of primary tumors rather than secondary tumors, but elbow prosthesis reconstruction after tumor resection is a viable option for primary and secondary bone malignancies (Casadei, 2016). Li (2016) in a literature review reported limb salvage surgery is an optimal treatment for osteosarcoma. Kadam (2013) feels limb salvage is the choice of procedure versus amputation in 95% of limb sarcomas without affecting patient survival.
Once a tumor has been removed, limb reconstruction begins. This may involve replacing major vessels, performing muscle transfers, and doing plastic surgery reconstruction. Replacement of a large segment of missing bone is challenging. This sometimes includes allograft bone replacement using cadaver bone (figure: cadaver allograft; figure: fibular mandibular reconstruction). The native bone partially grows into the allograft and partially replaces it. Rejection is rare, but there are a number of complications including graft fracture and failure of healing between the graft and the native bone. With any type of orthopedic surgery, infection is always a possibility.
Limb sparing surgery has been revolutionized by metallic endoprostheses which replace joint surfaces and large segments of lost bone around a joint, particularly in the knee, shoulder, and elbow. At first, these prostheses were costumed made for the individual patient (figure: distal ulnar reconstruction; figure: limb sparing hemiarthroplasty; figure: limb sparing prosthesis; figure: varus-valgus limb sparing prosthesis). Nowadays, they are also available as routine products from major orthopedic device manufacturers (figure: DePuy Synthes limb preservation system).
Limb salvage surgery in the context of the present discussion mainly refers to limb reconstruction after resection of a bone or soft tissue sarcoma. However, in a larger context it can include discussion of limbs threatened by metastatic tumor and by large and small vessel disease, such as the effects of diabetes on the lower extremity. Limb salvage can also be discussed in the context of major arterial or venous injury or traumatic disfigurement of a limb (mangled limb) by a severe civilian or wartime injury.
Limb salvage is also sometimes needed for severe infections or significant failure of an earlier joint prosthesis (figure: infected total elbow arthroplasty; figure: distal radioulnar joint reconstruction). An infected knee prosthesis may be removed and a temporary prosthesis constructed out of antibiotic impregnated bone cement placed for several weeks to stabilize the joint space and allow antibiotic to leach into the infected tissues (figure: antibiotic impregnated cement temporary TKA). Once the infection at the joint site has been eliminated, a permanent revision prosthesis can be placed.
A broader look at limb salvage surgery is beyond the scope of the present discussion which is somewhat focused on limb sparing orthopedic prostheses. While these devices have significantly improved the survival and quality of life for multiple patients, they are subject to many complications, and there is usually a long rehabilitation period for any type of limb sparing treatment (Sevelda, 2015). Despite seemingly successful limb salvage, some patients elect late amputation for a variety of reasons, including complex pain, neurological dysfunction, infection, and unwillingness to endure a complicated course of treatment (Covey, 2015). Sometimes, arthrodesis or a similar more routine surgery provides the best treatment rather than a complex prosthesis (Ettinger, 2016). Nevertheless, limb salvage surgical techniques will continue to improve with better vascular, neurological, and soft tissue reconstructions, newer prostheses, and the introduction of tissue regeneration techniques.
Back to Top
Back to Top
|