by Tim B. Hunter, MD and Mihra S. Taljanovic, MD, PhD
No matter the body opening, there are individuals who will attempt to insert something into it themselves or allow others to insert a foreign object into it. The rectum, vagina, urethra, nose, and ear are favorite sites for insertion of foreign objects. These types of insertions are most frequently seen in children, but adult patients may derive sexual pleasure from it, be mentally incompetent, or do it merely out of curiosity (Table) (figures: foreign body insertions I).
Foreign Body Insertions: general principles
Category
Description
General Principles
Most insertions cause no harm
Minor mucosal injuries are common
Retained objects may be encrusted with mineral salts
Retained objects may perforate and travel to distant sites
Predisposed Patients
Children (especially those with emotional problems)
mentally incapacitated individuals
adults engaging in "unusual" sexual activities
patients undergoing surgery or instrumentation
patients undergoing non-traditional medical therapy
Complications
Severe bleeding from mucosal injury
edema preventing natural passage or easy removal
organ perforation with hemorrhage, abscess formation, or sepsis
Bladder foreign bodies are particularly prone to being a site for deposition of mineral salts with the formation of one or more bladder calculi (figure: bladder calculus) (Lebowitz, 1987). In fact, a bladder calculus in a child or young adult should raise the suspicion of an encrusted foreign body.
Surprisingly, most foreign bodies inserted into the urethra or rectum do not cause significant injury even if they are large, sharp, or pointed (figures: foreign body insertions II). These tubular structures are capable of considerable expansion, and they are well lubricated by natural fluids. Patients also learn how to “dilate” these structures so that they will accommodate large objects (figure: milk can in rectum; figure: traffic wand in rectum). The most common complications of a rectal foreign body are retention and rectal bleeding. The most serious complication is perforation either related to the foreign body insertion or the attempts to remove it (Yildiz, 2013).
Common rectal foreign bodies that result from medical procedures going awry include thermometers, rectal tubes, anal packs, light covers, enema tips and covers, suppository wrappers, and oral or topical medication used inappropriately in the rectum (Zelegman, 1986).
The supine view of the abdomen is often the first radiograph obtained to evaluate a patient with abdominal or pelvic pain with or without a history of foreign body insertion. If the object lies in the bladder, it will generally be oriented mediolaterally. If it lies in the vagina or rectum, it will generally be oriented craniocaudally. This rule is probably more applicable in children than in adults, because vaginal foreign objects may lie mediolaterally in adults. Oblique and lateral radiographs of the pelvis as well as endoscopy and cross-sectional studies (mainly ultrasound and CT) can help determine the exact location of a foreign body. CT is recommended if a colonic foreign body is proximally located or cannot be removed manually (Maddu, 2014).
Cleansing enemas are sometimes a source of complications for patients. There can be mucosal injury from the enema fluid being too hot or too caustic. The enema tube or its protective sheath may be retained in the rectum or sigmoid or the mucosa may be lacerated and perforated. Small, retained colonic foreign bodies usually pass spontaneously. Large ones may induce enough wall edema or bowel atony that they cannot be passed naturally. In such instances, they must be removed endoscopically; by perianal extraction with the patient under anesthesia; or surgically, with either direct removal of the object from the bowel or with laparotomy and anal removal of the object (Richter, 1975; Wolf, 1977; Effaiha, 1977).
Retained rectal bodies may rarely form asymptomatic calcified fecaliths. More commonly, they cause acute and chronic discomfort and can produce severe bleeding, bowel obstruction, and perforation. Retained objects can also ascend higher into the colon, even as far as the hepatic flexure. If they perforate the colon, they may lodge in the retroperitoneal tissues, induce localized contained abscesses, lie free within the peritoneum, or even travel to distant sites in the body (Effaiha, 1977; Lau, 1981; Morales, 1983; Buzzard, 1979).
The nose is a common location for children to insert foreign bodies, such as coins. The nasal mucosa can become swollen making removal of the foreign object difficult. Not infrequently, more than one foreign body has been inserted into the nose, and radiography may be necessary for proper evaluation of a potential nasal foreign body (ies) and to assure their successful removal. In any case, careful physical examination of the nose as thoroughly as is reasonably possible is recommended to determine the presence and number of foreign bodies inserted as well as to determine their later successful removal.
Button magnets can be especially pernicious foreign bodies if inserted into the nose, particulary if a button magnet is inserted into both sides of the nose (figure: button magnets in the nose) (Kazikdas, 2017). They may strongly magnetically adhere to each other leading to nasal mucosal injury and severe bleeding, even mucoperichondral erosion of the nasal septal cartilage.
Young child who had placed a screw in her vagina. From Hunter, 1994
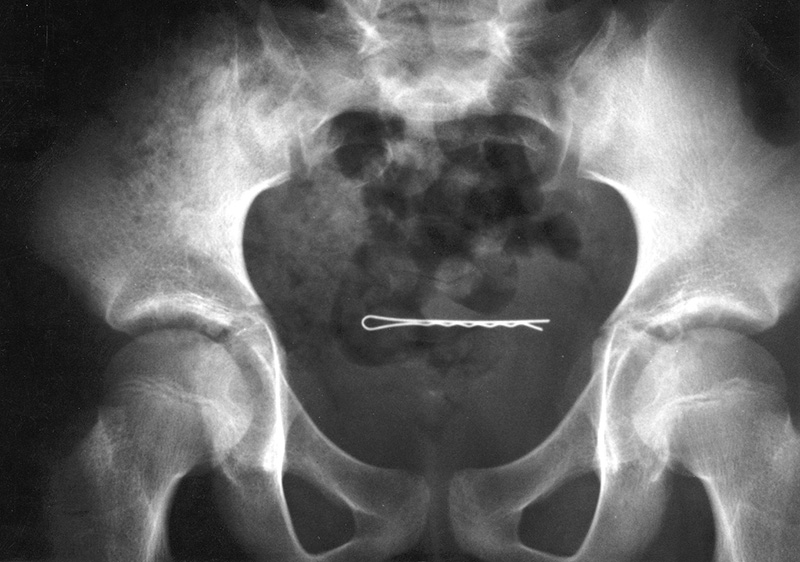
A 2 year-old girl had placed a bobby pin in her bladder (Courtesy George Barnes, MD). From Hunter, 1994
Young man who had inserted a pen refill in his urethra with partial rupture of the urethra and soft tissue gas in the penis. (Courtesy Laurie L Fajardo, MD). From Hunter, 1994
15 year-old boy with a broken rectal thermometer lying free in the peritoneum. Its origin was unknown. He denied inserting any foreign objects into his rectum or urethra. He had had no treatments or hospitalization since he was one year old. (Courtesy George Barnes, MD). From Hunter, 1994
Bobby pin in uterus
Umbilical and labial rings
Wire in bladder
Condensed milk can in rectum
19 year-old woman with a bobby pin lodged in her uterus. She had attempted to induce an abortion with the bobby pin. A subsequent self-induced abortion was successful. (Courtesy George Barnes, MD). From Hunter, 1994
Young woman with multiple "piercings" including an umbilical ring and labial rings.
18 year-old man with bladder calculi that formed around a wire in his bladder. Six months prior he lost a fine telephone wire in his bladder when he achieved an erection while inserting the wire into his urethra during masturbation. (Courtesy George Barnes, MD). From Hunter, 1994
60 year-old man with a condensed milk can that he had inserted into his rectum. (Courtesy George Barnes, MD). From Hunter, 1994
Foreign Body Insertions: figures II
Traffic wand in rectum
25 year-old man who sat on a dildoa
Drinking glass in the rectum
Cigarette lighter in the rectum
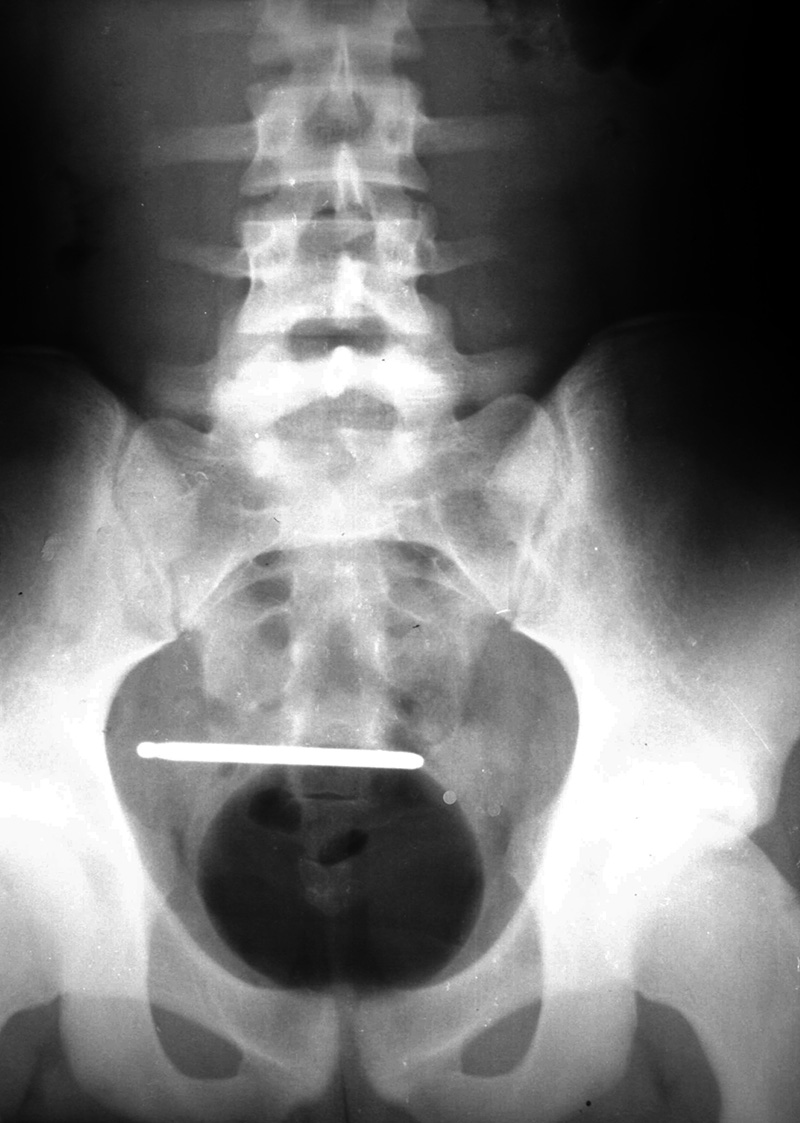
Policeman who somehow lost his traffic wand in his rectum. From Hunter, 1994
51 year old man with bottle of gargling fluid in his Hartman pouch which had been placed three weeks previously after he had distal colon surgery to remove an impacted shampoo bottle. (Courtesy Tyler Gibb, MD)
Image courtesy Benjamin W Strong, MD.
11 year-old boy had inserted button magnets in each side of the nose 6 hours previously. They were removed with the help of household magnets after the patient was taken to the operating room and placed under general anesthesia (from Kazikdas, 2017)