Normal whole body pediatric and adult bone scintigraphy with technetium 99m methylene diphosphonate (MDP) display different features (figure 1). In the pediatric population there is intense radiotracer uptake in the growing physes of long bones. Normal adult whole body planar bone scans with Tc-99m MDP demonstrates normal expected uptake in the bilateral sacroiliac joints, iliac crest, acromioclavicular joints, sternoclavicular joints, and nasal region. Normal radiotracer activity is excreted into the kidneys and urinary bladder.
While FDG is an analog of glucose, the fluoride in NaF incorporates into the hydroxyapatite (mineral component) of bone by replacing a hydroxyl group to form fluoroapatite. F18-NaF PET bone scan commonly demonstrate non-malignant, scattered focal uptake within the spine, bilateral knees, feet and shoulder joints, consistent with degenerative bone remodeling. Normally, there is no brain uptake on NaF PET scanning.
| Figure 1A |
Figure 1B |
Figure 2A |
Figure 2B |
 |
 |
 |
 |
| Normal pediatric whole body Technetium 99m-methylene diphosphonate (Tc-99m MDP) bone scan displays intense expected radiotracer uptake in the physes of long bones. |
Normal adult whole body bone scan Tc-99m MDP demonstrates normal expected uptake in the bilateral sacroiliac joints, iliac crest, acromioclavicular joints, sternoclavicular joints and nasal region. Normal radiotracer activity is excreted into the kidneys and urinary bladder. |
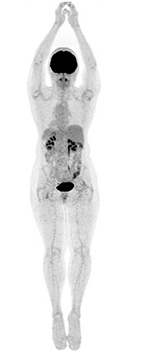
A) Whole-body F18-FDG PET scan maximum intensity projection (MIP) bone demonstrates intense uptake in the brain and renal excretion. Mild activity is seen within the bone marrow. B) Whole-body F18-NaF PET bone scan maximum intensity projection (MIP) demonstrates scattered focal uptake within the spine, bilateral knees, feet and shoulder joints consistent with degenerative bone remodeling. Note: Intense uptake is seen within the brain on FDG PET and no uptake is seen on NaF PET. |
 |
| Figure 3 |
Figure 4A |
Figure 4b |
Figure 5A |
 |
 |
 |
 |
| Tc-99m MDP bone scan shows photopenic defects involving bilateral knee joints in the region of femoral and tibial condyles. |
A) 50 year-old women with history of osteosarcoma of left distal femur status post resection and limb sparing prosthesis. B) Left to right, top to bottom, axial bone window CT and FDG PET, fused axial and coronal images of the lower thigh demonstrate the prosthesis within the distal left femur producing streak artifact and photopenia on the PET images. |
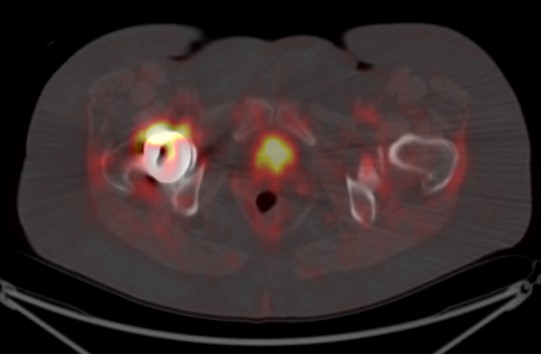
60 year-old women with right hip hemiarthoplasty. Axial CT bone window image (5A) demonstrates right hip prosthesis. |
|
| Figure 5B |
Figure 5C |
Figure 5D |
Figure 5E |
 |
 |
 |
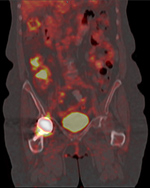 |
| Axial bone window (5B) NON-attenuation corrected (NAC) and attenuation corrected (AC) FDG PET (5C), fused axial and coronal (5D, 5E), images of the pelvis demonstrate the right femoral prosthesis with photopenia in the region of prosthesis. Periprosthetic FDG uptake is seen on AC and fused images and is minimally seen on the NAC image, consistent with attenuation correction artifact. |
|
| Figure 6A |
Figure 6B |
Figure 6C |
Figure 7A |
 |
 |
 |
 |
| 49 year-old women with right hip hemiarthroplasty. Maximum intensity projection images of CT with bone window (A), NaF PET (B), and fused PET-CT image (C) demonstrate right femoral prosthesis with intense NaF uptake in the proximal femur surrounding the prosthesis, representing reparative bone remodeling. This can last for years and is not pathological. |
15 year-old girl with history of osteosarcoma of left femur status post resection and prosthesis. Lateral (A) and AP (B) radiographs of the left knee show a distal femur limb sparing prosthesis and knee arthroplasty. |
|
| Figure 7B |
Figure 7C |
Figure 7D |
Figure 8A |
 |
 |
 |
 |
| 15 year-old girl with history of osteosarcoma of left femur status post resection and prosthesis. Lateral (A) and AP (B) radiographs of the left knee show a distal femur limb sparing prosthesis and knee arthroplasty. |
15 year-old girl with history of osteosarcoma of left femur status post resection and prosthesis. Tc99m whole body bone anterior (C) and posterior (D) projections at different window settings demonstrate mild diffuse increased radiotracer activity around the distal end of the femur prosthesis and proximal end of tibial prosthesis, representing reparative bony remodeling. This can last for many years and is not pathological unless patient complains of new pain in which case one should consider loosening, infection, or recurrence of tumor. |
40 year-old man with history of facial trauma, status post mandibular reconstruction. A mandibular radiograph (A) demonstrates mandibular reconstruction on the right side with loss of bone and teeth. Tc-99m MDP (B) bone scan demonstrates uptake within the body of mandible on the left side which is due to altered stress from chewing. |
|
| Figure 8B |
|
|
|
 |
|
|
|
| 40 year-old man with history of facial trauma, status post mandibular reconstruction. A mandibular radiograph (A) demonstrates mandibular reconstruction on the right side with loss of bone and teeth. Tc-99m MDP (B) bone scan demonstrates uptake within the body of mandible on the left side which is due to altered stress from chewing. |
|
|
|
| |
|
|
|