| Dislodgement of cervical spine posterior fixation rods |
Fracture of spinal fixation rods |
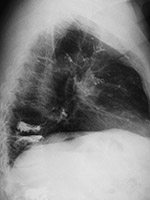
Pantopaque in the base of the cranium |
 |
 |
 |
 |
| 59 year-old man with past history of C3-5 fractures and extensive posterior spinal fixation from the occiput to T8. Lateral radiographs of the cervical spine three months apart show dislodgement (arrow) of the bilateral cervical posterior rods from connection with the thoracic rods at the C7-T1 level. Left: before dislodgement. Right: after dislodgement. After dislodgement there is increased kyphosis at the C6-7 level. |
From Hunter, 2004 |
Residual Pantopaque in the base of the cranium from a myelogram performed with Pantopaque many years prior. From Hunter, 1994 |
 |
| Failure of posterior cervical fusion |
|
|
 |
 |
|
|
| 68 year-old woman with posterior spinal fixation extending from the occiput to C3 involving posterior elements of C2 and C3 (left image). The surgery was performed for unstable atlantoaxial subluxation after remote cervical spine trauma. CT imaging follow-up (right image) demonstrated the C2 and C3 fixation screws were posteriorly displaced into the spinal musculature. |
|
|
|
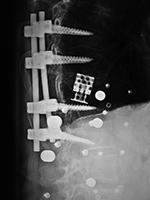
| Vertebroplasty at L1 and L3 |
Embolization of vertebroplasty cement into the pulmonary arterial tree
|
 |
 |
 |
 |
There is extrusion of vertebroplasty cement into the T12-L1 disk space.
|
From Hunter, 2004a |
|
| Expandable corpectomy cage |
Expandable corpectomy cage Sagittal CT image |
Expandable corpectomy cage after cage shift |
Displaced pedicle screw nut |
 |
 |
 |
 |
| 75-year old woman with expandable corpectomy cage used to treat a comminuted T11 compression fracture (left and center images). A follow-up study 3 months after cage placement (right image) shows cage shift probably from increased fracture compression. The cage remained stable at that point. |
|
|
| Failure of interlaminar lumbar instrumental fusion (ILIF) |
Posterior cervical fusion incorrect screw placement |
 |
 |
 |
 |
| 85 year-old woman with ILIF at L4-5. There is a bone plug and interspinous clamp. On lateral radiographs the spondylolysthesis at L4-5 increases from extension to flexion indicating partial failure of the fusion. |
64 year-old man with trauma and cervical spine degenerative disease. The C4-6 posterior screws enter into the facet joints. |
|
| Subsidence of PEEK cage device 3 months after surgery |
Anterior Cervical Disk fusion with junctional disease above the level of fusion |
 |
 |
 |
 |
| An anterior cervical fixation plate and screws has been placed with PEEK disk cages at C5-6 and C6-7. |
Three months after surgery the disk cage at C6-7 has subsided and slipped anteriorly. |
The radiograph on the left was obtained on February 11, 2013. That on the right was obtained on July 22, 2015. It shows degenerative changes developing at the C4-5 disk space above the anterior fusion going from C5-7. |






































