| Fixation screw projecting into right hip joint |
Left first metatarsophalangeal joint arthrodesis screw fractures |
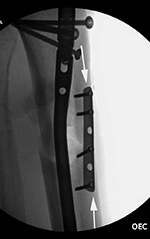
Left tibia stress fracture after fibular fracture fixation |
 |
 |
 |
 |
| The compression screw has slid distally in the barrel as it was designed to do when the femoral neck fracture site becomes compressed. This did not prevent the screw from cutting out of the femoral head (curved arrow). From Hunter, 1994 |
52 year-old man with chronic wound on plantar surface of the left foot and poliomyelitis of the left 2nd metatarsal head (arrow). There is incidental fracturing of two fixation screws from past large toe MTP joint arthrodesis. |
A short one-third tubular plate and screws plus interfragmentary screw stabilize a healing distal fibular fracture. An associated stress fracture (arrow) is in the distal tibial metaphysis from altered weight-bearing from the fibular fracture. |
 |
| Right femur periarticular plate breakage and chronic fracture nonunion |
Iatrogenic fracture fixation failure |
 |
 |
 |
 |
| 36 year-old man with bullet wound in 2003 complicated by femur fracture infected non-union treated by multiple attempts with external fixation and open reduction and internal fixation (ORIF). Radiography 12 years later shows chronic fracture hypertrophic nonunion, multiple shrapnel fragments, and breakage of a periarticular fixation plate. |
Intraoperative fixation of an intertrochanteric fracture demonstrates a cephalomedullary device with the tip of the cephalic screw positioned too short and very inferior in the neck (very large tip-apex distance). |
Subsequent fracture fixation failure observed as the head and neck segment of the femur flexed 90 degrees with cut-out of the screw approaching the hip joint. |
|
| Failure of fracture fixation due to ambulating against advice |
 |
 |
 |
 |
| Male patient with proximal tibia and fibula fractures treated by intramedullary nail and supplemental one-third tubular plate. Initial intraoperative fluoroscopic AP and lateral images (left two images) show the plate (arrow on lateral image). The patient ambulated against advice and was lost to follow-up. Two months later he again presented (right two images) to the clinic. There is now tibia fracture migration, and the proximal medial to lateral interlocking screw has backed out (AP view). The lateral view demonstrates fracture displacement with flexion deformity. The nail has troughed outside the proximal anterior tibia and is sitting within the soft tissues. The supplementary plate is broken, there is a broken interlocking screw, and abundant fracture callus is present. |
|
| Left hip cannulated screw fracture |
Left knee antegrade intramedullary rod displacement into knee joint |
Left ankle syndesmotic screw fracturing |
 |
 |
 |
 |
| 41 year-old man with chronic left femoral neck fracture and fracture of superior cannulated fixation screw. The partially visualized intramedullary nail is for an old femoral shaft fracture. |
|
|
22 year-old man with syndesmotic screw placement for medial avulsive ankle injury. The screws fractured and loosened and were later removed. |




































{kind=link}